Open Access | Research
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Results of transurethral augmentation urethroplasty for stricture of fossa navicularis
* Corresponding author: Ibragim E. Mamaev
Mailing address: N.I. Pirogov Russian National Research Medical University, V.M. Buyanov Moscow City Clinical Hospital, Moscow, Russia.
Email: dr.mamaev@mail.ru
Received: 19 January 2026 / Revised: 12 February 2026 / Accepted: 27 February 2026 / Published: 31 March 2026
DOI: 10.31491/UTJ.2026.03.053
Abstract
Background: Stricture of the distal urethra is an actual problem due to the complexity of surgical correction
methods capable of providing a high-level aesthetic and functional result. In this regard, we used a new method that meets the above requirements.
Methods: A prospective study of the treatment outcome was conducted in 12 patients with distal urethral
stricture at the Moscow City State hospital V.M. Buyanov from 2021 to 2025. The inclusion criterion was the
presence of isolated urodynamically significant narrowing of the urethra in the area of the fossa navicularis. All
patients underwent transurethral ventral urethrotomy of the narrowed area with optical control of the depth
of transection. Subsequently, a triangular fragment of the oral mucosa was taken and fixed in the urethra using the “inlay” technique using 4 sutures (4-0 monocryl) deep in the urethra and 5-7 sutures along the ventral
semicircle of the external opening. Restoration of independent urination was achieved on the 12-14th day.
Results: The average age of the patients was 65.5 years. The observation period ranged from 7 to 54 months.
The etiologic factor was lichen sclerosus in 8 cases and iatrogenic stricture in 4 patients. The labial mucosa
was used as a graft in 9 patients, and the buccal mucosa in 3 patients. No intra and postoperative complications
were noted. Average urination quality indicators before surgery: uroflowmetry Qmax 6.12 ± 3.62; IPSS 20.92 ±
6.22. After surgery, Qmax 15.60 ± 4,63; IPSS 7 [4.00; 13.25]. No patient reported urine splashing during urination. All patients were satisfied with the aesthetic result of the surgery. The surgeon’s subjective assessment of
the convenience of using grafts from the lip and cheek was in favor of the lip mucosa.
Conclusion: The method of transurethral augmentation plastic surgery of the distal urethral stricture using
the oral mucosa is an effective and safe method for correcting obstruction of this etiology. The use of the labial
mucosa is preferable because of the smaller thickness of the graft. It also preserves the buccal mucosa in patients with lichen sclerosus for possible future reconstruction.
Keywords
Urethral stricture, meatal stenosis, fossa navicularis stricture, augmented urethroplasty
Introduction
Urethral stricture (US) is a narrowing of the urethra due
to scarring of the urethral mucosa with varying degrees
of spongiofibrosis. This disease is one of the causes of
the development of lower urinary tract symptoms in men
and leads to deterioration in the quality of life (QoL). The
incidence of urethral stricture is 0.6% [1]. The possibilities of conservative treatment of dysuric symptoms in
this disease are very modest. If a moderate effect on the
symptoms of accumulation is possible, then the symptoms
of emptying associated with stricture of the urethra do not
change in any way against the background of drug treatment. The only effective method of treating patients with
US is surgical intervention. The choice of surgical treatment method depends on the location, extent, etiology of
the urethral stricture, as well as on the preservation of the
urethral site.
The localization of urethral stricture in the fossa navicularis relative to other parts of the urethra is relatively low
and amounts to 18% [2]. Nevertheless, this problem is especially relevant due to the need for the surgeon to solve
two tasks during treatment: the formation of an adequate
lumen of the urethra and ensuring a good cosmetic result.
In addition, there are high requirements for the persistence
of a positive result, including because lichen sclerosus is a
common (42%) etiological factor of stricture of the fossa
navicularis of the urethra. Being a progressive variant of
corpus spongiosum damage, it causes a high incidence of
US recurrence [3]. The purpose of the study is to evaluate
the efficacy and safety of transurethral ventral augmentation of the urethra in men with fossa navicularis stricture.
Methods
A prospective study was conducted at the V.M. Buyanov Moscow City Clinical Hospital to evaluate the treatment results of 12 patients with fossa navicularis stricture of the urethra who underwent transurethral augmentation urethroplasty from 2021 to 2025. The criterion for inclusion in the study was the presence of a urodynamically significant narrowing of the urethra in the fossa navicularis. To determine the indications for surgery, standard methods of examination and evaluation of urination parameters were used: uroflowmetry, filling out IPSS and QoL questionnaires, determination of residual urine, retrograde and micturition urethrocystography. The control study 6 months after surgery included uroflowmetry and filling out the IPSS questionnaire, QoL.
The technique of performing transurethral augmentation plastic surgery of the fossa navicularis of the urethra
The patient is placed on the operating table in a supine
position. Under endotracheal anesthesia, suture holders
are applied on the sides of the external opening of the urethra to open the meatus. A spear-shaped scalpel inserted
through the external opening of the urethra is used to longitudinally dissect the stricture of the fossa navicularis of
the urethra at 6 o’clock on the conventional dial from the
external opening of the urethra to the proximal border of
the stricture. The lumen of the urethra during dissection is
supported by vascular tweezers inserted into its distal part.
An endoscope is used to perform urethroscopy, which
evaluates the depth and length of the incision, as well as
the size of the required graft. The urethra is calibrated by
passing a 26 Ch metal urethral bougie through the area of
the dissected urethra to a depth of 4-5 cm.
After marking and hydrotreating with a 1:200,000 epinephrine solution in a volume of 10 mL, a triangular graft
of the required size is taken from the mucous membrane
of the inner surface of the lower lip or cheek according to
the standard procedure. Hemostasis of the graft bed is performed.
Under the control of an endoscope, by puncturing the
skin from the ventral surface of the penis, a needle with
a thread (17 mm, ½, Monocryl 4-0) is inserted into the
lumen of the urethra along the proximal border of the
urethrotomy incision, captured by a needle holder and
removed from the urethra. The tip of the triangular flap is stitched with a needle removed from the urethra, after
which the needle is reinserted into the urethra and punctured from the inside out at the point of primary injection.
Further, by light traction for the applied thread, the flap
is immersed into the formed area, while the flap is maintained in a straightened state due to the threads previously
applied to its corners. After immersion in the urethra, the
ligature is tied. The wide part of the graft is compared
with the external opening of the urethra along the ventral
semicircle in the dissection area by applying 5-7 nodular
sutures (Monocryle 5-0). According to a technique similar
to the one described above, the center and sides of the triangular graft are fixed under optical control of the needle
being guided from the outside into and out of the urethra.
A silicone urethral catheter 12-16 Ch is inserted into the bladder (Figure 1).
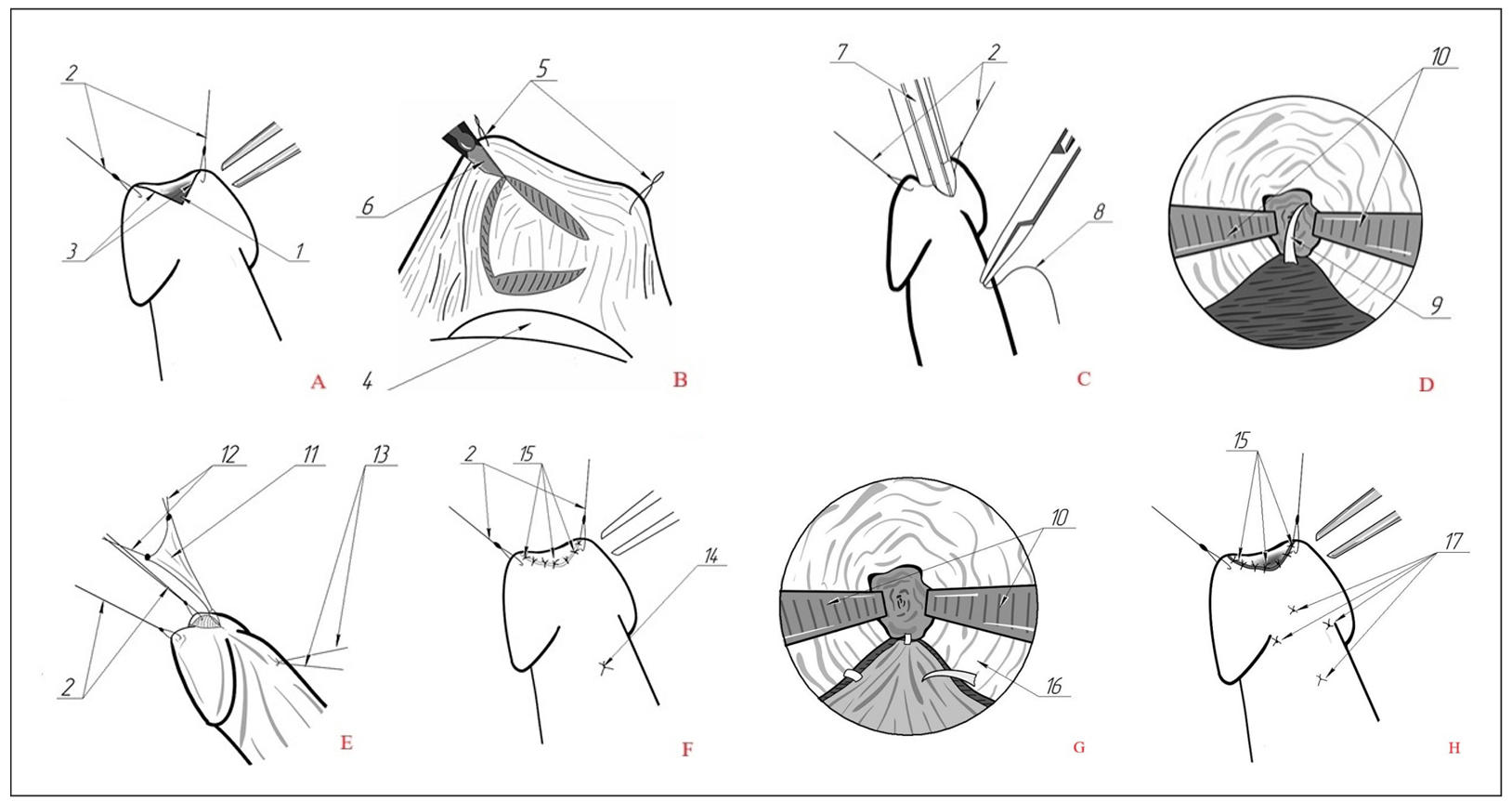
Figure 1. Stages of transurethral augmentation urethroplasty of the fossa navicularis of the urethra. (A) ventral urethrotomy, formation of an augmentation site. (B) the labial graft fence. (C) needle injection for subsequent ligation. (D) optical control of the injection point in the area of the proximal angle of the urethrotomy incision. (E) insertion of the graft into the urethra onto the formed site by traction of the ligature. (F) the final appearance of the penis after surgery. 1: ventral meatotomy. 2: stitches-holders. 3: the edges of the dissected urethra. 4: a gauze cloth placed at the base of the lower lip to push back the tongue. 5: stitches-holders. 6: scalpel. 7: endoscope. 8: application of the first suture on the proximal edge of the dissected urethra. 9: visualization of the needle during endoscopic examination. 10: tweezer branches. 11: labial graft. 12: stitches-holders at the corners of the triangular graft. 13: threads superimposed on the proximal edge of augmentation. 14: node on the proximal edge of augmentation. 15: nodular sutures on the distal edge of augmentation (meatus). 16: the edge of the urethral mucosa. 17: fixing seams on the top and sides of the triangular graft from the outside.
Statistical analysis
The organization and statistical data processing were performed using Microsoft Office Excel 2010 (Microsoft Corp., Redmond, WA, USA) and the STATISTICA v.7.0 program (StatSoft Inc., Tulsa, OK, USA). All anamnestic, clinical, laboratory, and instrumental data were entered into a Microsoft Excel database developed by the author and processed using variational statistics. The data was analyzed for compliance with the normal distribution law using the Kolmogorov-Smirnov criterion. For quantitative data with a normal distribution, the arithmetic mean (M) and standard deviation (SD) were used, which were represented as M ± SD. If the quantitative data did not follow the law of normal distribution, the median (Me), lower and upper quartiles (Q1 – Q3) were used to describe them. The indicators were compared using the Student ttest for data with a normal distribution. In the absence of a normal distribution, the Mann–Whitney U-test was used. A threshold of P = 0.05 was used to determine statistically significant differences. Sensitivity and specificity were calculated with a 95% confidence interval.
Results
All 12 patients underwent transurethral augmentation urethroplasty of the fossa navicular using the “ventral inlay”
technique. The material for augmentation in 3 cases was
the mucous membrane of the cheek and in 9 cases the mucous membrane of the lip. The median age of the patients
was 65.5 years. The etiological factor of urethral stricture
in 8 cases was lichen sclerosus, in 4 cases the stricture was
of an iatrogenic nature (underwent TUR of the prostate
gland/catheterization of the bladder). The average length
of the urethral stricture was 20.83 ± 7.93 mm. The maximum length of the urethral stricture is 35 mm. There were
no intra and postoperative complications. All patients had
a urethral catheter inserted for 14 days to drain the lower
urinary tract. The follow-up period ranged from 7 to 54 months.
The results of the surgical intervention are shown in Table 1. The average value of the maximum urination rate (Qmax)
before surgery according to uroflowmetry was 6.12 mL/s.
The median of score on the IPSS questionnaire before surgery was 21.5 points, and the average value of QoL was
4.67 points. The median of volume of residual urine (VRU)
before surgery was 35 mL. After surgery, the average Qmax
value was 15.6 mL/s; the median of IPSS score was 7; the
average QoL score was 1.92; the median of volume of residual urine value was 5 mL.
Table 1.
Urodynamic and clinical results of transurethral ventral inlay augmentation urethroplasty of the fossa navicularis.
| Indicator | Before urethroplasty | After urethroplasty | P |
|---|---|---|---|
| Qmax, mL/s* | 6.12 ± 3.62 | 15.10 ± 4.89 | < 0.001 |
| IPSS, point* | 20.92 ± 6.22 | 11.00 ± 7.08 | 0.003 |
| QoL, point* | 4.67 ± 0.98 | 2.17 ± 1.47 | < 0.001 |
| VRU, mL** | 35 [18,75; 59,5] | 0 [0; 20] | 0.092 |
Note: Qmax: maximum urination rate; IPSS: International Prostate Symptom Score; QoL: quality of life; VRU: volume of residual urine. *Average value, standard deviation. **Median, lower and upper quartiles.
Splashing of urine during miction after surgery was not
noted by any patient. All patients were satisfied with the
aesthetic result of the operation.
During the follow-up period, we recorded a recurrence
of urethral stricture in one case. In a patient with lichen
sclerosus as an etiological factor, a recurrence of stricture of the same localization and extent was detected 16
months after the initial surgical intervention. In this case,
dorsal inlay buccal grafting of the navicular fossa was
performed. At the time of writing, three months after the
second surgical intervention, there was no recurrence of
urethral stricture in this patient.
Even despite the identified recurrence of urethral stricture
in a single case, when conducting a statistical analysis of
the results obtained among all patients who underwent
surgery, we revealed a statistically significant improvement in the quality of urination. 6 months after urethroplasty, an endoscopic assessment of the surgical area was
performed by urethroscopy with a rigid urethrocystoscope
16 Ch. According to the results of the study, the surgical
intervention area was freely passable for the instrument
in all but one patient. In a single case of recurrence, we
noted a narrowing of the fossa navicularis to 6 Ch.
Discussion
Currently, there are many different methods of surgical
treatment of stricture of the distal urethra, which include various options for urethroplasty, as well as meatotomy
and urethral dilatation.
Minimally invasive techniques such as urethral dilatation
and internal optical urethrotomy cannot be considered
radical treatment methods and often lead to relapse. During urethral dilatation, the narrowed area expands due to
lacerations of scar tissue and healthy mucosa, which leads
to an aggravation of the process and an increase in the degree of narrowing of the urethra and the length of the urethral stricture. Performing an internal optical urethrotomy
in the penile urethra is technically difficult due to the difficulty of providing a lever for manipulating the instrument.
In addition, such an operation carries a potential risk of
unintentional injury to the corpus cavernosum and glans
penis, which can lead to intraoperative bleeding, and in
the long term to erectile dysfunction [4]. We have not been
able to find studies in the modern literature evaluating
the effectiveness of urethral dilatation and internal optical
urethrotomy in penile stricture of the urethra. A systematic
review published by Veeratterapillay R. et al. shows that
for urethral strictures of all localizations, the effectiveness of urethral dilatation and internal optical urethrotomy
ranges from 10% to 90% [5]. According to available data,
the effectiveness of internal optical urethrotomy is most
effective in carefully selected patients with primary nontensioned stricture of the bulbous urethra [4, 6].
Meatotomy is a common, effective and long-used method
of treating distal strictures of the urethra. However, this
technique is used only in cases of narrowing of the urethra
limited by the external opening of the urethra. J. Meeks
et al. presented the results of meatotomy performed in 74
patients, among whom 86% of operations were considered
successful [3]. Despite satisfactory postoperative urination
parameters, this technique has a number of disadvantages:
due to ventral meatotomy, a meatus similar to hypospadias
is formed, which is a cosmetic defect; when performing
dorsal meatotomy, there is a risk of intraoperative bleeding; a number of patients experience urine splashing during injection in the postoperative period [7].
For fossa navicularis stricture in combination with meatostenosis, it is possible to perform an extended meatomy
(stage 1 of the Johanson operation), during which the skin
of the penis and urethra is dissected along the ventral surface, followed by a comparison of the mucous membrane
of the urethra and the skin of the penis. The effectiveness
of this method reaches 87% [8]. In addition, this technique
allows not only to enlarge the lumen of the urethra, but
also to simultaneously excise the fibrotic tissue of the urethra. This fact allows the use of extended meatotomy as
the first stage of complex treatment and allows for further
augmentation urethroplasty. The literature also describes
the opinion that extended meatotomy for lichen sclerosus
allows access to the disease site for topical corticosteroid
therapy, which can potentially reduce the likelihood of lichen sclerosus progression [7]. However, due to the similar standard ventral meatotomy technique, the described technique has the same disadvantages [8].
The most effective ways to treat patients with fossa navicularis stricture of the urethra are various urethroplasty
techniques. There are two fundamentally different types of
urethroplasty: replacement and augmentation. In the first
case, a complete excision of the altered section of the urethra is performed and the urethral pad is formed using a
graft or flap, followed by tubularization of the urethra in a
delayed period. Augmentation urethroplasty involves enlarging the lumen of the urethra using “insertion” or “lining” techniques. Reconstructive materials for performing
urethroplasty surgery are most often: the mucous membrane of the oral cavity, the skin of the preputial sac or the
skin of the penis. They may have a vascular pedicle as a
source of blood supply (flap), or they may not have their
own source of blood supply (graft). Currently, the cheek
mucosa is considered a universal transplant [7], however,
to date, no studies have been conducted comparing the
results of reconstruction of distal strictures of the urethra
using various oral cavity transplants, such as the mucous
membrane of the cheek, lip or tongue.
The methods of urethral skin grafting are well known to
the world urological community. B. Cohney can be considered a pioneer of this approach. In 1963, he described
the technique of augmentation urethroplasty of the fossa
navicularis of the urethra with a skin flap of the penis,
during which a flap formed from the skin of the inferior
lateral surface of the penis is transposed onto the lower
surface of the dissected urethra [9]. In 1967, J. Blandy et
al. demonstrated a new technique of Y-V skin meatoplasty
[10]. With the accumulation of experience and long-term
results, it became obvious that these techniques do not
provide patients with the desired cosmetic and functional
results [7]. The technique to avoid the disadvantages inherent in the methods described above was developed and
presented to the world community by G. Jordan in 1987.
A distinctive feature of this technique is the use of a distal
skin fascial islet flap of the penis. This approach made it
possible to augmentation of the entire stricture zone up to
the external opening of the urethra, which made it possible
to avoid significant cosmetic defects of the penis [11]. R.
Virasoro et al. conducted a prospective study of a group
of patients who underwent Jordan meatoplasty. The work
showed that of the 39 patients under observation, 29 (83%)
had an excellent result with a median follow-up of 10.2
years. Recurrence of urethral stricture was recorded in 6
cases, and all of these patients had lichen sclerosus [12].
These data confirm the generally accepted opinion about
the low effectiveness of skin urethroplasty among patients
with lichen sclerosus. These data confirm the generally
accepted opinion about the low effectiveness of cutaneous
urethroplasty among patients with sclerotrophic lichen. In
another study performed by Morey et al. the effect of the
length of the urethral stricture on the recurrence rate after
undergoing a single-stage skin graft surgery was analyzed.
According to the data published by the authors, the desired result was achieved in 91% of patients with a distal
urethral stricture of less than 2.5 cm, while with a stricture
of more than 2.5 cm, a recurrence was registered in 54%
[8].
The best long-term results are demonstrated by various
variants of augmentation urethroplasty with a buccal graft.
The classic technique for correcting the stricture of the
fossa navicularis of the urethra is the “dorsal insert” technique, in which the skin of the penis and urethra is longitudinally dissected along the ventral surface from the external opening of the urethra proximally to healthy tissues.
Next, a longitudinal dissection of the dorsal surface of the
urethra is performed in order to form a graft site. After
graft fixation, the ventrally dissected urethra is sutured,
then the skin of the penis above it is sutured [13]. According to the results of a series of such operations, D. Dubey
et al. demonstrated 88% success among 24 patients with
fossa navicularis stricture with an average follow-up time
of 26.6 months [13]. Another surgical treatment method is
buccal ventral onlay urethroplasty of the fossa navicularis.
Similarly to the first stage of the dorsal inlay technique, a
longitudinal dissection of the urethra is performed along
the ventral surface, after which a rectangular graft is fixed
to the edges of the dissected urethra, and the skin incision
is sutured [14]. P. Chowdhury et al. demonstrated the results of treating 6 patients with fossa navicularis stricture
using this method. In half of the cases, lichen sclerosus
was the etiological cause of US, while the other 50%
were iatrogenic in nature. The average length of the stricture was 1.5 cm. With a median follow-up of 37 months
in 83% of patients, the result was considered successful
based on improved urodynamic parameters [14].
To date, there is no consensus among specialists on which
approach to reconstruction is preferable for distal urethral
strictures. A lot of data from various studies with varying
effectiveness of one- and two-stage reconstructive interventions with various grafts and flaps have been published
in the medical literature. For example, D. Dubey et al.
analyzed the incidence of recurrence of urethral stricture
after buccal urethroplasty in patients with lichen sclerosus. In the course of the study, the authors revealed that
performing two-stage urethroplasty is associated with
a higher recurrence rate (21.4%) compared with singlestage (12%) [15]. However, it is worth noting that the
implementation of augmentation techniques is possible
only if the urethral pad is preserved. In case of urethral
obliteration or significant spongiofibrosis, two-stage
urethroplasty is justified. D. Dubey et al. also compared
the effectiveness of buccal urethroplasty using the dorsal
onlay technique with skin graft urethroplasty using the
dorsal onlay technique. The authors obtained comparable
data on the recurrence rate: 10.1% for buccal and 14.4%
for cutaneous urethroplasty. However, patients’ satisfaction with the treatment results was higher in the buccal
urethroplasty group (89% to 65%) [15].
In 2022, R. Farrell et al. published an analysis of a fiveyear experience of transurethral dorsal augmentation
urethroplasty for fossa navicularis stricture. The intervention consisted in the fact that after dorsal dissection of the
external opening of the urethra, a triangular buccal graft
was placed in the formed incisional defect, fixing its tip to
the proximal border of the incision, and the distal face to
the edge of the dissected external opening. A total of 16
patients were operated on by the authors using this technique, all of them achieved a good functional result and
in 94% of cases the anatomical result was also regarded
as good [16]. The disadvantage of the technique is the difficulty of correcting stricture, the length of which exceeds
1.5 cm, since full-fledged fixation of the graft in the depth
of the urethra along the dorsal surface is technically difficult.
A similar method of transurethral buccal urethroplasty
using the ventral insertion technique is described by M.
Daneshvar et al. The essence of the technique is to dissect the external opening of the urethra and the stricture
of the fossa navicularis from the urethra, during which a
wide lumen is formed without dissecting the skin of the
penis. The next step is to take a triangular buccal graft and
place the latter in the area of the dissected urethra. To do
this, a suture is applied to the tip of the triangular graft
and the proximal edge of the dissected urethra is stitched
through with the same thread under endoscopic control.
By traction by the thread, the graft is delivered to the site
formed during dissection, the knot is tied and the graft
base is fixed to the external opening of the urethra [17].
The absence of a cutaneous incision provides a number
of advantages: maximum preservation of blood supply in
the reconstruction area, elimination of the risk of ventral
urethrocutaneous fistula formation, and excellent cosmetic
results. The absence of a skin incision is especially important in the treatment of patients with the etiological factor
of lichen sclerosus, since it is generally believed that this
disease is characterized by the presence of the Koebner
phenomenon, which consists in the appearance of new lesions and progression at the sites of skin injury [18, 19].
The authors of the technique describe the results of treatment of 68 patients with stricture of the fossa navicularis
of the urethra. n the study, surgeons performed an operative manual according to the original technique for a patient with a median length of urethral stricture of 2 cm. In
34% of cases, the etiology of the disease was lichen sclerosus. With a median follow-up of 17 months, the absence
of relapse was noted in 95% of cases [17].
Based on the above-described technique of transurethral
buccal urethroplasty of the fossa navicularis [17], we performed urethroplasty of the fossa navicularis of the urethra in 12 patients. For the first three patients, the cheek
mucosa served as an augmentation material. In the course
of our research, we suggested greater ease of operation
and, possibly, better long-term results when using a labial
graft. In this connection, it was decided to perform urethroplasty of the fossa navicularis of the urethra in subsequent patients using the lip mucosa. According to the
authors of this publication, the labial graft, in comparison
with the buccal graft, due to a thinner layer of the submucosal base, makes it easier to straighten the graft in the
reconstruction area and provides a better cosmetic result.
An additional factor in favor of labial graft is the preservation of the cheek mucosa, which may be required for
further reconstruction in case of recurrence or progression
of US. Another important feature of our technique, which
distinguishes it from the original one, is the application
of additional fixing sutures along the lateral edges of the
graft, which allows us to be sure of the straightening and
corrects orientation of the graft in the urethra.
Conclusions
The technique of transurethral augmentation urethroplasty of the fossa navicularis of the urethra is an effective, safe and relatively easily reproducible method of stricture correction, which allows achieving excellent functional results. The mucous membrane of the lower lip is a convenient and reliable material for transurethral augmentation of distal strictures of the urethra. It provides excellent cosmetic results and allows you to preserve the buccal mucosa in case subsequent reconstructions are necessary.
Declarations
Author contributions
Mamaev I.: study concept, study design development, data acquisition, data analysis, scientific editing, supervision; Alekberov E.: literature review, data acquisition, data analysis, statistical data processing; Kotov S.: study concept, study design development, critical review, scientific editing, supervision.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
All authors declared that there are no conflicts of interest.
Ethical approval and informed consent
The study was approved by the Local Independent Ethics Committee of Pirogov Russian National Research Medical University (RNRMU) (Protocol No. 234 dated November 20, 2023).
References
1. Santucci R, Joyce G, & Wise M. Male urethral stricture disease. J Urol, 2007, 177(5): 1667-1674. [Crossref]
2. Fenton A, Morey A, Aviles R, & Garcia C. Anterior urethral strictures: etiology and characteristics. Urology, 2005, 65(6): 1055-1058. [Crossref]
3. Meeks J, Barbagli G, Mehdiratta N, Granieri M, & Gonzalez C. Distal urethroplasty for isolated fossa navicularis and meatal strictures. BJU Int, 2012, 109(4): 616-619. [Crossref]
4. Tonkin J, & Jordan G. Management of distal anterior urethral strictures. Nat Rev Urol, 2009, 6(10): 533-538. [Crossref]
5. Veeratterapillay R, & Pickard R. Long-term effect of urethral dilatation and internal urethrotomy for urethral strictures. Curr Opin Urol, 2012, 22(6): 467-473. [Crossref]
6. Kotov S, Belomytsev S, Surenkov D, Pulbere S, Guspanov A, Yusufov E, et al. Internal optical urethrotomy: effectiveness and its place in modern urology. Experimental and Clinical Urology, 2017, 2017 (No.2): 112-116.
7. Singh S, Agrawal S, & Mavuduru R. Management of the stricture of fossa navicularis and pendulous urethral strictures. Indian J Urol, 2011, 27(3): 371-377. [Crossref]
8. Morey A, Lin H, DeRosa C, & Griffith B. Fossa navicularis reconstruction: impact of stricture length on outcomes and assessment of extended meatotomy (first stage Johanson) maneuver. J Urol, 2007, 177(1): 184-187; discussion 187. [Crossref]
9. Cohney B. A penile flap procedure for the relief of meatal stricture. Br J Urol, 1963, 35: 182-183. [Crossref]
10. Blandy J, & Tresidder G. Meatoplasty. Br J Urol, 1967, 39(5): 633-645. [Crossref]
11. Jordan G. Reconstruction of the fossa navicularis. J Urol, 1987, 138(1): 102-104. [Crossref]
12. Virasoro R, Eltahawy E, & Jordan G. Long-term follow-up for reconstruction of strictures of the fossa navicularis with a single technique. BJU Int, 2007, 100(5): 1143-1145. [Crossref]
13. Dubey D, Kumar A, Mandhani A, Srivastava A, Kapoor R, & Bhandari M. Buccal mucosal urethroplasty: a versatile technique for all urethral segments. BJU Int, 2005, 95(4): 625-629. [Crossref]
14. Chowdhury P, Nayak P, Mallick S, Gurumurthy S, David D, & Mossadeq A. Single stage ventral onlay buccal mucosal graft urethroplasty for navicular fossa strictures. Indian J Urol, 2014, 30(1): 17-22. [Crossref]
15. Dubey D, Vijjan V, Kapoor R, Srivastava A, Mandhani A, Kumar A, et al. Dorsal onlay buccal mucosa versus penile skin flap urethroplasty for anterior urethral strictures: results from a randomized prospective trial. J Urol, 2007, 178(6): 2466-2469. [Crossref]
16. Farrell M, Campbell J, Zhang L, Nowicki S, & Vanni A. Transurethral reconstruction of fossa navicularis strictures with dorsal inlay buccal mucosa graft urethroplasty. World J Urol, 2022, 40(6): 1523-1528. [Crossref]
17. Daneshvar M, Simhan J, Blakely S, Angulo J, Lucas J, Hunter C, et al. Transurethral ventral buccal mucosa graft inlay for treatment of distal urethral strictures: international multi-institutional experience. World J Urol, 2020, 38(10): 2601-2607. [Crossref]
18. Pugliese J, Morey A, & Peterson A. Lichen sclerosus: review of the literature and current recommendations for management. J Urol, 2007, 178(6): 2268-2276. [Crossref]
19. Zhang X, Lei L, Jiang L, Fu C, Huang J, Hu Y, et al. Characteristics and pathogenesis of Koebner phenomenon. Exp Dermatol, 2023, 32(4): 310-323. [Crossref]