Open Access | Case Report
This work is licensed under a Creative
Commons Attribution-ShareAlike 4.0 International License.
Torsion of a cryptorchidism testicle in a toddler
* Corresponding author: Shahid Ali
Mailing address: Shalamar medical and dental college, Lahore, Pakistan.
Email: imshahiduro@gmail.com
Received: 30 December 2023 / Revised: 02 February 2024 / Accepted: 20 February 2024 / Published: 27 March 2024
DOI: 10.31491/UTJ.2024.03.017
Abstract
Undescended testis and testicular torsion are rare clinical entities. Symptoms can be confusing and may be interpreted as signs of other more common conditions. Furthermore, late recognition of undescended testis can significantly delay diagnosis and lead to adverse outcomes. Here we present the case of a 2-year-old toddler who presented with painful right-sided groin swelling and an empty scrotal sac. Intraoperatively, a torsion of the undescended testis was confirmed and an orchiectomy of the right testis and an orchidopexy of the left side were performed. This case report also highlights the importance of early diagnosis of testicular torsion and prompt surgical intervention.
Keywords
Orchiectomy, testicular torsion, urological emergency, orchidopexy
Introduction
Cryptorchidism or undescended testis is the absence of one or both testes in their normal position in the scrotal sac. It may be
palpable or non-palpable [1, 2]. While previous
reports of testicular torsion in cryptorchidism suggest that this is an entity seen in patients with neuro-muscular disorders,
torsion of an undescended testis can be seen in normal children. Because the likelihood of salvage of a torsioned testis is strongly
associated with the duration of torsion, it is important that the emergency medicine community be aware of the presenting
characteristics and imaging findings of testicular torsion. To date, there are few reports of torsion of the undescended testis in
normal children in the literature. In this case report, we present a case of testicular torsion of the undescended testis in an
otherwise normal toddler and briefly review the relevant literature to further highlight this urologic emergency
[3-5].
Testicular torsion occurs when the testicle twists, resulting in decreased blood flow to the affected testicle. Testicular
torsion is most common between the ages of 10 and 25. If not treated in time, the blood supply to the testicle may be completely
reduced, leading to ischemia, necrosis, and death of the testicle. This is an emergency condition and immediate surgical repair
can result in testicular salvage. The testicular salvage rate is approximately 100 percent if surgery (untwisting of the testis) is
performed within 6 hours; the salvage rate drops to 20 percent if surgery is delayed for 24 hours
[3, 4].
There are two types of torsion of the testis, it can be intravaginal or extravaginal. Extravaginal torsion of the testis is most
common in neonates. The attachment of the tunica vaginalis to the scrotal wall is inadequate or still developing in early infancy,
which accounts for the higher likelihood of bilateral torsion in this age group. With increasing age, as the attachment of the
tunica becomes stronger, the incidence of this type of torsion decreases
[1, 5].
Intravaginal torsion is most commonly seen in older children and adults, and the known anatomical abnormality responsible for it is
the Bell-Clapper malformation. Normally, the tunica vaginalis completely surrounds the testis except for the epididymis and the
posterior scrotal wall. In Bell-Clapper malformation, there is a high investment of the tunica vaginalis on the testis, which
allows rotation of the spermatic cord within the sac, leading to intravaginal torsion of the testis. This malformation is bilateral
and therefore justifies bilateral exploration and fixation of both testes even in cases of unilateral testicular torsion
[1-3].
Case report
A 2-year-old toddler with a known history of bilateral cryptorchidism presented to our emergency department with fussiness,
right groin swelling, pain, and decreased movement of the right leg. He was a full-term, otherwise healthy infant. Prior to the
current presentation, he had been evaluated at an outside hospital for right groin pain, vomiting, and low-grade fever and was
discharged home with oral antibiotics and analgesics. He continued to do poorly, and his parents noticed decreased movement in
his right leg, so they brought him to our hospital for reevaluation. Examination revealed an extremely tender, edematous, indurated,
and erythematous area along the right inguinal canal and no palpable testes bilaterally in the scrotum. The scrotum was poorly
developed and empty.
Ultrasound of the inguinoscrotal region showed an empty scrotal sac. The right testis was seen in the right inguinal canal
measuring 15×12×8 mm with a volume of 0.7 mL. This also shows paratesticular heterogeneity with possible early mass-like
morphology. The left testis was seen in the left inguinal canal measuring 12×10×6 mm with a volume of 0.4 mL, without
paratesticular mass formation or epidydimal enlargement.
Right testicular tumor was suspected and testicular tumor markers were sent. Emergency right inguinal exploration was performed
(Figure 1 & 2). The right testis was firmly
adherent to the surrounding tissues in the inguinal canal. Intraoperatively, a necrotic right testis with torsion of the
spermatic cord was found. The patient underwent right orchiectomy and left orchidopexy.
Testicular tumor markers were normal. The histopathology report shows features consistent with infarction (post-torsion). At
follow-up, the patient was healthy and well. The wound site was clean and the dressing was intact.
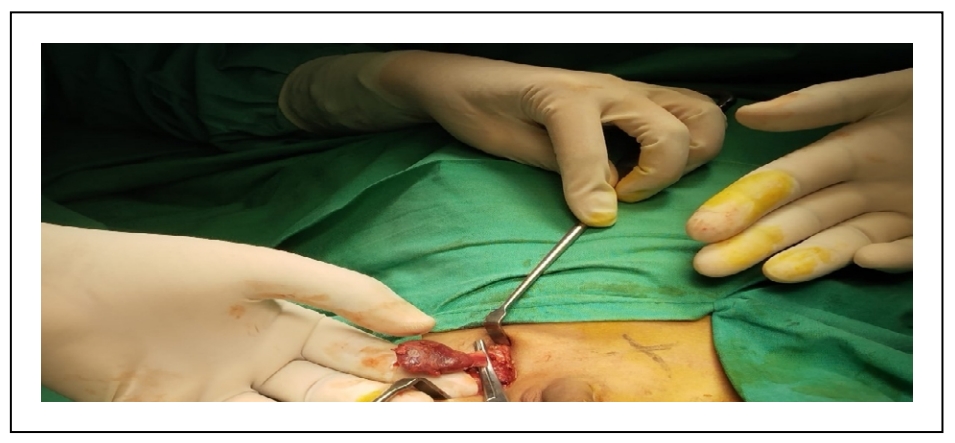
Figure 1. Intra-operative findings of non-viable testis on right side.

Figure 2. Right sided orchiectomy.
Discussion
Cryptorchidism or undescended testis (a testis that does not descend into the scrotum) is the most common genitourinary
condition in newborn males. Normal descent of the testis into the scrotum usually occurs between 25 and 35 weeks of intrauterine
life. The rate of diagnosis of undescended testis at birth is 1-4% in term infants and up to 45% in preterm infants. Most cases of
undescended testis descend voluntarily into the scrotum by 3 months of age. Descending testis is also possible after 3 months of
age. In some premature infants, the testes do not descend or disappear into the abdomen until full term. In a few cases, testes
that were present in the scrotum descend again after birth. The process of normal testicular descent, testicular re-accession,
and testicular recurrence is not fully understood. Approximately 1-2% of boys older than 6 months of age develop an undescended
testis after its initial postnatal descent. Undescended testes are known to be associated with increased rates of malignancy and
decreased fertility. Prompt referral to urology and timely surgical correction may improve fertility rates and decrease malignancy
rates associated with undescended testes [4-6].
Torsion of the testis is a common urological emergency in the pediatric population. It can be divided into two types based on the
mechanism of onset: "intravaginal" and "extravaginal". Approximately 90% of torsion cases are classified as intravaginal,
indicating that the torsion occurred within the tunica vaginalis. This often occurs in the setting of Bell-Clapper malformation,
in which the tunica vaginalis, instead of reflecting off the epididymis, covers the epididymis and spermatic cord, leaving the
testis free to hang and move in the scrotum. Intravaginal torsion is most common in older children and adults. Extravaginal
torsion is often seen in newborns and indicates twisting of the spermatic cord outside of the tunica vaginalis
[1, 3, 5].
Impalpable testis and an inguinal mass on the ipsilateral side are the classic presentation and should raise the suspicion of
torsion of the undescended testis. Urgent Doppler ultrasound can lead to a correct and prompt diagnosis in most cases: the affected
testis is swollen, may show heterogeneous and absent signals on Doppler ultrasound. The twisted spermatic vessels may show a whirl
sign on Doppler. Although differentiating undescended testicular torsion from incarcerated hernia can be challenging and
misdiagnosis may occur, both require immediate surgical exploration via an inguinal approach
[7].
The "golden window of opportunity" to salvage testicular function after the onset of symptoms has been suggested to be 4 to 8
hours, as failure to intervene within this time decreases testicular function and increases the rate of removal of the testes
(orchiectomy). Retrospective data from 558 children from Croatia showed the importance of early presentation and surgical
correction within 6 hours was associated with a testicular salvage rate of 90-100%, whereas children presenting 6 to 12 hours and
12 to 24 hours after symptom onset had salvage rates of 20-50% and 0-10%, respectively. However, early presentation is a
well-documented and critical step in increasing testicular preservation rates [3,
4, 8].
In our opinion, the above case is an important learning point for many reasons. First, the intraoperative findings, the scrotal
examination, and the absence of bilateral testes indicate that the diagnosis of undescended testis had eluded routine clinical
examination for years. Had the diagnosis been made earlier, the testis could have been returned to the scrotal position and this
presentation could have been avoided. The above highlights the importance of clinical awareness among clinicians (e.g.,
pediatricians and general practitioners) who typically perform routine examinations in early childhood and, most importantly,
education of patients and their caregivers. Unfortunately, lack of awareness among healthcare professionals and patients has been
associated with delayed presentation and adverse outcomes. In addition, the need for clinical examination must be emphasized. The
presence of pain and a mass in the groin with an empty scrotum should immediately raise the suspicion of an undescended testis. A
thorough physical examination contributes significantly to the early diagnosis of torsion [9].
Conclusions
Torsion of the undescended testis is a relatively rare entity in the normal child. However, because the likelihood of testicular
preservation is strongly correlated with the duration of torsion, it is advisable that all physicians, especially those who see
patients in the emergency setting, be aware of this emergency condition. Inguinal swelling with an ipsilateral empty scrotum should
raise suspicion of torsion of the undescended testis and further evaluation with Doppler ultrasonography and urologic consultation
should be performed.
In this particular case, there was marked twisting of the right spermatic cord and the testis was ischemic and necrotic. Right
orchiectomy and left orchidopexy were performed. The histopathology report shows features consistent with infarction
(post-torsion). At follow-up, the patient was healthy and well.
Declarations
Financial support and sponsorship
None.
Conflict of interest statement
No conflict of interest.
Ethical Approval and Informed consent
The patient has provided an informed consent for publication of images and information in this study.
References
1. Pal DK, Tiwari AK, & Choudhury S. A rare case of simultaneous bilateral testicular torsion in inguinal canal: a case report. Journal of Pediatric and Adolescent Surgery, 2020, 1(2): 95-97. [Crossref]
2. Cohen S, Gans W, & Slaughenhoupt B. Acute scrotum. American Urological Association Guidelines, 2021.
3. Reddy K, Ramteke H, Patel DJ, Deshpande SG, Patil M, & Nayak K. Testicular torsion and irreversible loss in an adolescent male: a harrowing case report with emphasis on timely intervention and literature review. Cureus, 2023, 15(7): e42754. [Crossref]
4. Komarowska MD, Pawelczyk A, Matuszczak E, Dębek W, & Hermanowicz A. Is testicular torsion a real problem in pediatric patients with cryptorchidism? Front Pediatr, 2020, 8: 575741. [Crossref]
5. Guo BC, & Wu HP. Atypical symptoms of testicular torsion in a 7-year-old child: a case report. Medicine, 2023, 102(18): e33709. [Crossref]
6. Shin J, & Jeon GW. Comparison of diagnostic and treatment guidelines for undescended testis. Clin Exp Pediatr, 2020, 63(11): 415-421. [Crossref]
7. Kargl S, & Haid B. Torsion of an undescended testis - a surgical pediatric emergency. J Pediatr Surg, 2020, 55(4): 660-664. [Crossref]
8. Shunmugam M, & Goldman RD. Testicular torsion in children. Can Fam Physician, 2021, 67(9): 669-671. [Crossref]
9. Reed B, Banerjee R, Tsampoukas G, & Gray R. Testicular torsion in an undescended testicle: chasing a diagnosis. J Surg Case Rep, 2022, 2022(6): rjac263. [Crossref]