Open Access | Research
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Effects of structured group reminiscence in sports and non-sports environments on cognitive empowerment and optimism in older adults: a quasi-experimental study
* Corresponding author: Bahador Azizi
Mailing address: Faculty of Sports Sciences, Ferdowsi University of Mashhad, Mashhad, Iran.
Email: bahador.azizi@mail.um.ac.ir
Received: 31 March 2025 / Revised: 08 April 2025/ Accepted: 17 May 2025 / Published: 27 June 2025
DOI: 10.31491/APT.2025.06.174
Abstract
Background: Research indicates that engaging in various activities
and exercising in a green outdoor environment offers numerous psychological and
physiological benefits, particularly for the older adults, when compared to indoor
or non-sport environments. Therefore this study aimed to investigate the impact
of structured group reminiscence on cognitive empowerment and optimism in older
adults, addressing the need for effective interventions to promote successful aging.
Methods: A quasi-experimental pretest-posttest design was employed,
involving 36 older adults (aged 60–79) selected via convenience sampling. Participants
were randomly assigned to either a reminiscence group in a sports environment, a
reminiscence group in a non-sports environment, or a control group (12 participants
in each group). The intervention were conducted once weekly for 12 weeks, each session
lasting 60 to 90 minutes. Cognitive empowerment was measured using the Older Adults
Cognitive Empowerment Questionnaire, and optimism was assessed using the Optimism (Life
Orientation) Questionnaire.
Results: The multivariate analysis of the covariance (MANCOVA)
revealed significant improvements in cognitive empowerment (P < 0.05) and optimism
(P < 0.05) post-test scores in both reminiscence groups (sports and non-sports
environments) compared to the control group. There was a trend toward greater
gains in the sports environment group, although this difference was not statistically
significant.
Conclusion: Structured group reminiscence, regardless of the environment,
is an effective intervention for enhancing cognitive empowerment and optimism in older adults.
These findings suggest that incorporating reminiscence therapy into programs for older adults
can contribute to improved psychological well-being and successful aging. Further research is
warranted to explore the potential benefits of sports environments in maximizing the effects
of reminiscence therapy.
Keywords
Reminiscence, older adults, cognitive empowerment, optimism, sports environment, aging
Introduction
Population aging is a global phenomenon. In 2020, an estimated 727 million older adults
were living worldwide. All nations are witnessing a rapid expansion in their aging populations,
with projections suggesting that by 2050, this number will double to exceed 1.5 billion [1].
The growing population of older adults is contributing to a higher prevalence of age-related
health challenges [2, 3]. As a result, nations are confronted with significant obstacles in
ensuring their healthcare and social support systems are equipped to address this demographic
shift [4]. Aging is inherently linked with complex conditions such as declining physical
health and loss of autonomy, both of which are associated with adverse mental health outcomes.
Furthermore, psychosocial stressors, including loneliness, bereavement, diminished income,
and societal changes, may exacerbate mental health challenges in older adults, ultimately
diminishing their quality of life [5].
Active aging emphasizes the empowerment of older adults across biological, psychological,
and social domains. Empowerment, in this context, encompasses fostering self-improvement,
autonomy, self-confidence, alignment with personal values, and the ability to assert one's
rights and freedoms [6, 7]. Consequently, in recent years, the concept of patient empowerment
has gained a pivotal role in nursing and medical research. It is now regarded as an essential
component of nursing practice [8, 9], necessitating efforts to enhance individuals' intrinsic
understanding and awareness of the aging process [7]. Additionally, some studies have
conceptualized empowerment through a social lens, emphasizing the importance of social
connections and services in fostering a sense of control and agency. Effective intervention
designs require a thorough understanding of the sociocultural contexts and characteristics
of the target population. From this perspective, participants are considered active agents
in the empowerment process. Interventions are less about modifying participants' behaviors
and more about unlocking human potential to achieve desired outcomes. The empowerment process
is context-dependent, rooted in the environmental and social framework, and is inherently a
collective process facilitated through collaboration with others [10].
Studies examining the empowerment of older adults have yielded valuable insights. For instance,
Musavi et al. identified seven dimensions of empowerment in the context of receiving social
support: obtaining information from family and others, receiving guidance from healthcare
professionals, managing disease risk factors, adhering to medication regimens, achieving
functional and mental independence, establishing meaningful relationships, and attaining
goal satisfaction [11]. Similarly, Khezri et al. developed a self-management competency
questionnaire tailored to older adults with hypertension, focusing on three domains:
knowledge, attitudes, and practices [12]. Figar et al. introduced an empowerment tool
grounded in the concepts of resource enhancement, capacity building, and knowledge
acquisition, which demonstrated efficacy in reducing systolic blood pressure [13].
DeCoster and George incorporated elements such as control, self-efficacy, vitality,
and competence in designing their empowerment instrument [14].
Numerous factors have been explored as indicators of successful aging,
with optimism emerging as a significant variable influencing individuals' beliefs
and experiences. Optimism, as a positive mediator, exerts its impact through
effective coping mechanisms, problem-solving strategies, information-seeking
behaviors, and positive reframing within psychological domains, including
social support and perceived control over life circumstances [15]. Seligman et al.
define optimism as a trainable cognitive pattern that equips individuals to confront
challenging situations more effectively [16, 17]. Additionally, optimism is considered
an inter-individual characteristic, reflecting the degree to which individuals hold
favorable and general expectations about their future. From a psychological standpoint,
this distinction among individuals is of considerable importance [18].
Research indicates that older adults tend to exhibit less optimism about their
future compared to younger adults; however, optimism and positive expectations
increase significantly in later life, particularly around the age of 80 [19].
Optimistic individuals display adaptive behaviors, including psychological
resilience [20], enhanced psychological well-being [21], higher self-esteem [22],
lower levels of stress and exposure to negative events [23], and reduced mortality
rates associated with cardiovascular disease [24].
Reminiscence, one of the most widely utilized psychosocial interventions, has
demonstrated effectiveness in enhancing older adults' well-being. This process
involves recalling past memories and sharing life experiences to foster positive
emotions and coping strategies [5, 25]. A notable advantage of reminiscence is its
ability to bolster older adults' self-worth and identity through the recollection
of past experiences [26]. Moreover, reminiscence is a cost-effective and accessible
intervention that can improve cognitive functioning, social engagement, positive
emotions, personal identity, and overall quality of life. Reminiscence sessions typically
involve the use of evocative tools, such as old songs, photographs, and newspapers,
to stimulate memory recall [27].
Numerous studies have advocated for reminiscence-based interventions as an effective
strategy to enhance self-esteem [4, 27-30], alleviate anxiety [31, 32], reduce depressive
symptoms [31-36], mitigate loneliness [31, 37], improve insomnia and sleep quality [38],
increase happiness [39], foster spiritual well-being [38], promote positive self-concept [40],
and support emotional well-being [4]. These interventions have also been shown to enhance
mental health in older adults [27-30], elevate life satisfaction [33-35, 41, 42], and improve
quality of life [42, 43]. Reminiscence offers a compelling alternative to traditional
psychotherapies for promoting mental health among older adults and has been utilized as an
effective psychosocial intervention for over three decades [26, 44]. In a very recent study,
Eryılmaz et al. highlight the efficacy of group reminiscence therapy in non-clinical elderly
populations [45].
Environmental factors are another crucial determinant of mental health and its related
parameters, which are key indicators of quality of life [46]. Empirical evidence highlights
the potential synergy between the psychological benefits of physical activity and the
restorative effects of exposure to natural environments. Physical activity conducted in
natural settings may yield greater mental health benefits compared to activities performed
elsewhere. Substantial research and policy initiatives emphasize the role of natural
environments in safeguarding and enhancing human mental health [47]. Longitudinal studies
have identified social support from family or friends and interpersonal interactions as
pivotal social factors influencing mental health in older adults [48, 49].
In recent decades, the importance of the social and physical environment in shaping mental
health has garnered increasing attention. Residential neighborhoods play a significant role
in influencing health outcomes. Independent of individual or family characteristics,
neighborhood socioeconomic disadvantages are associated with premature mortality and poorer
physical and mental health outcomes [50-54]. Understanding the mechanisms linking these
associations is critical for improving public health and testing hypotheses about the influence
of broader social and contextual factors on psychological and biological functioning [55].
Neighborhood environments may impact health across the lifespan through diverse pathways,
including the provision of social services, promotion of health behaviors, exposure to
physical or material conditions, and social factors such as social support, social capital,
and social dysfunction [52-57]. Positive perceptions of neighborhood social
capital (e.g., social cohesion, interpersonal trust, and norms of reciprocity) are
consistently linked to a lower prevalence of mental health disorders, as evidenced by
cross-sectional and longitudinal studies conducted in the general population [58].
Although the relationship between neighborhood physical + environmental factors and mental
health has been less explored, studies suggest that perceptions of safety, access to parks,
and favorable neighborhood aesthetics are strong predictors of positive environmental
attributes. While most findings in this area are derived from cross-sectional studies,
some longitudinal evidence supports causal links between perceived safety, residential
density, and mental health [59, 60].
Given the critical role of the environment in shaping mental health and its implications
for well-being, as well as the principles of imagery in sports psychology—which advocate
for imagery practices to be conducted within sports environments for optimal effectiveness—it
can be posited that the unique characteristics of sports settings, including specialized
equipment, facilities, and social interactions, may contribute to enhancing individuals' empowerment
and sense of optimism. Considering the aforementioned factors, aging is often accompanied
by heightened vulnerability and challenges that can diminish life satisfaction and exacerbate
psychological difficulties. To better prepare older adults to navigate these transitions
successfully, research such as the present study is essential for identifying factors that
influence attitudes toward aging and its associated challenges. Hence, we hypothesized that
structured reminiscence therapy would significantly improve cognitive empowerment and optimism
in older adults. It is anticipated that the findings will provide actionable insights to
facilitate successful aging and help older adults overcome the challenges associated with
this stage of life more effectively.
Methods
Procedure
Men and women aged 60 to 79 years old took part in the present study. All participants were fully informed about the study’s objectives and the anonymous data collection procedures, and they provided written informed consent. Participants were randomly assigned to one of three groups: the reminiscence in a sports environment group (8 men and 5 women), the reminiscence in a non-sports environment group (7 men and 5 women), and the control group (7 men and 4 women). A quasi-experimental pretest-posttest design was employed; involving 36 older adults selected via convenience sampling. The study was executed in accordance with the rules laid down in the declaration of Helsinki and its later amendments. Also, this study was approved by the ethics committee of Islamic Azad University of Iran (Sari branch) (IR.IAU.SARI.REC.1403.409).
Participants
Eligibility criteria required participants to: Be between 60 and 79 years old. Not
engage in regular physical exercise (defined as any structured activity designed to
improve or maintain physical fitness, with guidelines recommending at least 150 minutes
per week of moderate-intensity aerobic activity along with muscle-strengthening exercises
on two or more days per week [61]). Obtain written permission from a doctor. Score below
a predetermined cut-off point on the baseline questionnaires. Have been registered in a
nursing home or been a regular park attendee for at least one year. Possess adequate cognitive,
visual, and auditory health. Not have experienced the loss of a relative or loved one during
the past six months.
Exclusion criteria were as follows: A diagnosis of Alzheimer’s disease. Presence of mental
disorders such as substance use disorder, dementia, Major depressive disorder (MDD), or
post-traumatic stress disorder (PTSD). Neurological disorders including seizures, Multiple
sclerosis (MS), or Parkinson’s disease. Significant cognitive, visual, or hearing impairments.
Attendance in less than 80% of the structured group reminiscence sessions. In total, 36 older
adults met these criteria and were able to comply with the study conditions.
Sample size calculations
A power analysis conducted with G*Power 3.1 software indicated that to detect a moderate effect size (f = 0.25) with an α-error of 0.05, power of 0.80, three groups, two measurement points, and an assumed correlation of 0.50 among repeated measures, at least 36 participants were required (i.e., 12 per group).
Cognitive empowerment
The Older Adults Cognitive Empowerment Questionnaire was used to assess older adults’ physical and mental ability. This questionnaire consists of eight dimensions: 1) physical ability; 2) self-esteem; 3) spirituality; 4) commitment; 5) role performance; 6) situational awareness; 7) self-management; and 8) self-assessment [59]. The items are scored from 0 to 50, in which 0 indicates the worst condition and 50 represents the best. In the present study, a score below 25 was defined as low cognitive empowerment, 25 to 37.5 represented moderate cognitive empowerment, and a score above 37.5 denoted high cognitive empowerment [62].
Optimism
The Optimism (Life Orientation) Questionnaire was used to assess older adults’ expectations of life outcomes and positive versus negative aspects. This questionnaire consists of two dimensions: 1) pessimism (including 3 items); and 2) optimism (including 3 items); Also 4 items are deviant that were removed during data analysis [63, 64]. The items are scored from 0 to 24, in which 0 indicates the worst condition and 24 represents the best. In the present study, a score below 12 was defined as low optimism, 12 to 18 represented moderate optimism, and a score above 18 denoted high optimism [63].
Intervention: the structured group reminiscence therapy
The structured group reminiscence therapy was performed once weekly for 12 weeks (three months), each session lasted one to one and a half hours. Sessions for the sports environment group were held in an outdoor park, and sessions for the non-sports environment group were held in a nursing house. The intervention that was implemented for the two experimental groups was the structured group reminiscence program used by [65]. In this program, 12 main topics were discussed in 12 weekly sessions. In each of these sessions, stimuli were used to recall memories related to the topic of the session, which, depending on the topic of the session, included photos, work tools, childhood toys, etc. The content of the whole structured group reminiscence intervention sessions is described in Appendix A.
Control condition
To control possible effects of social interaction with other participants or study personnel, the participants assigned to the control group gathered at a clinic. During this time, they could talk to each other and medical staff members. During this period, the control group received their usual care; of course, it was ensured that none of the participants in the control group participated in the structured group reminiscence program. It should be noted that during the study, there were no restrictions or changes in the daily life routine of participants in these three groups. They could continue their previous regular activities and programs of personal life.
Data analysis
All calculations were done by the SPSS software version 24. After data collection, the Kolmogorov-Smirnov test was conducted to check the normality of data distribution. Then, using Levene's test, the homogeneity of the variables was investigated in three groups. The multivariate analysis of the covariance (MANCOVA) was performed to identify and compare the effects of the structured group reminiscence program on each dependent variable, given that the influence of pre-intervention values on post-intervention ones was controlled in this study. In all the statistical tests, a P-value of 0.05 was considered indicative of significance. The effect size for MANCOVA was calculated using partial eta square (ηp2), with 0.01 ≥ ηp2 ≥ 0.059 indicating small effect, 0.06 ≥ ηp2 ≥ 0.139 indicating medium effect, and ηp2 ≥ 0.14 indicating large effect sizes [63].
Results
The experimental and control groups were homogeneous regarding age, marital status, and employment status. The mean age in the reminiscence in the sports environment, reminiscence in the non-sports environment, and control groups were 71.66, 70.89, and 71.32, respectively. Table 1 shows the mean and standard deviation of cognitive empowerment and optimism in the three study groups during the pre-test and post-test.
Table 1.
Mean and SD of cognitive empowerment and optimism in three groups during pre-test and post-test.
| Variable | Group | |||||
|---|---|---|---|---|---|---|
| Control | Reminiscence (non-sports environment) | Reminiscence (sports environment) | ||||
| Pre-test (M ± SD) | Post-test (M ± SD) | Pre-test (M ± SD) | Post-test (M ± SD) | Pre-test (M ± SD) | Post-test (M ± SD) | |
| Cognitive empowerment | 22.96 ± 3.87 | 26.62 ± 4.63 | 22.44 ± 4.36 | 48.36 ± 4.54 | 23.36 ± 4.43 | 52.76 ± 3.21 |
| Optimism | 8.16 ± 4.21 | 10.87 ± 5.36 | 9.35 ± 3.71 | 18.52 ± 5.69 | 9.25 ± 4.36 | 20.78 ± 4.44 |
Note: M = mean; SD = standard deviation.
As can be seen in Table 1, cognitive empowerment and optimism improved in both the sports and non-sports environment groups in the post-test compared to the pre-test, with these changes being more noticeable in the sports environment group. Also, to gain a clearer understanding of the groups' results in the pre-test and post-test, the comparisons of the groups' means based on cognitive empowerment and optimism are presented in Figure 1 and 2.
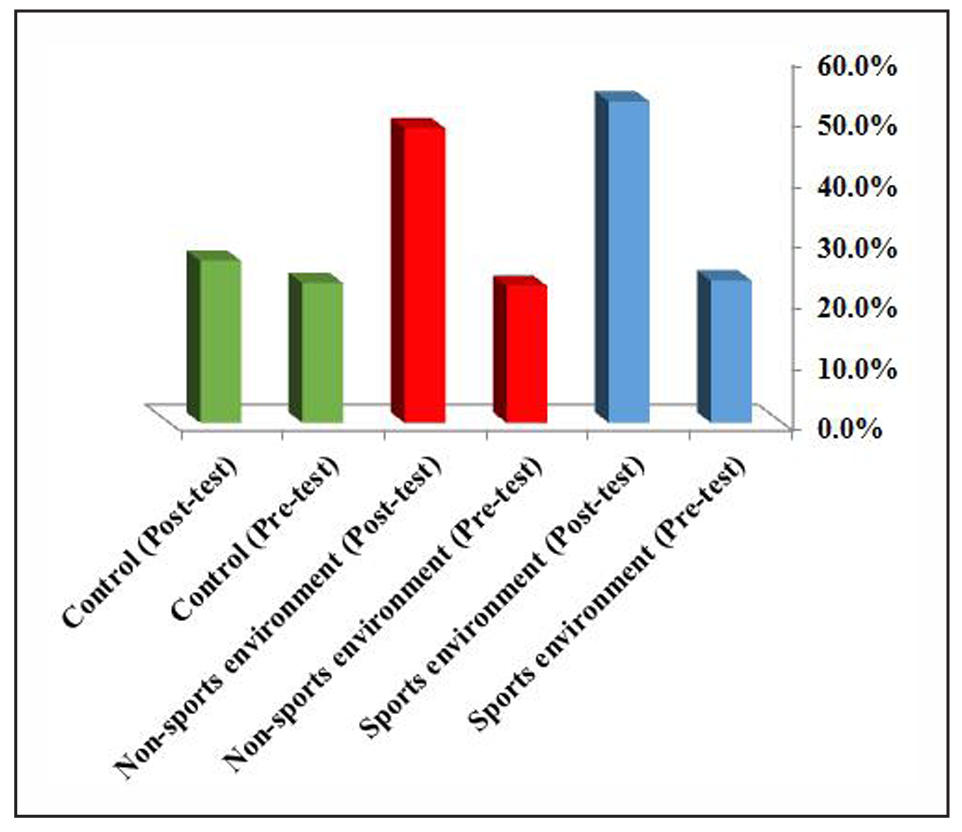
Figure 1. Results of groups' means based on cognitive empowerment in the pre-test and post-test.
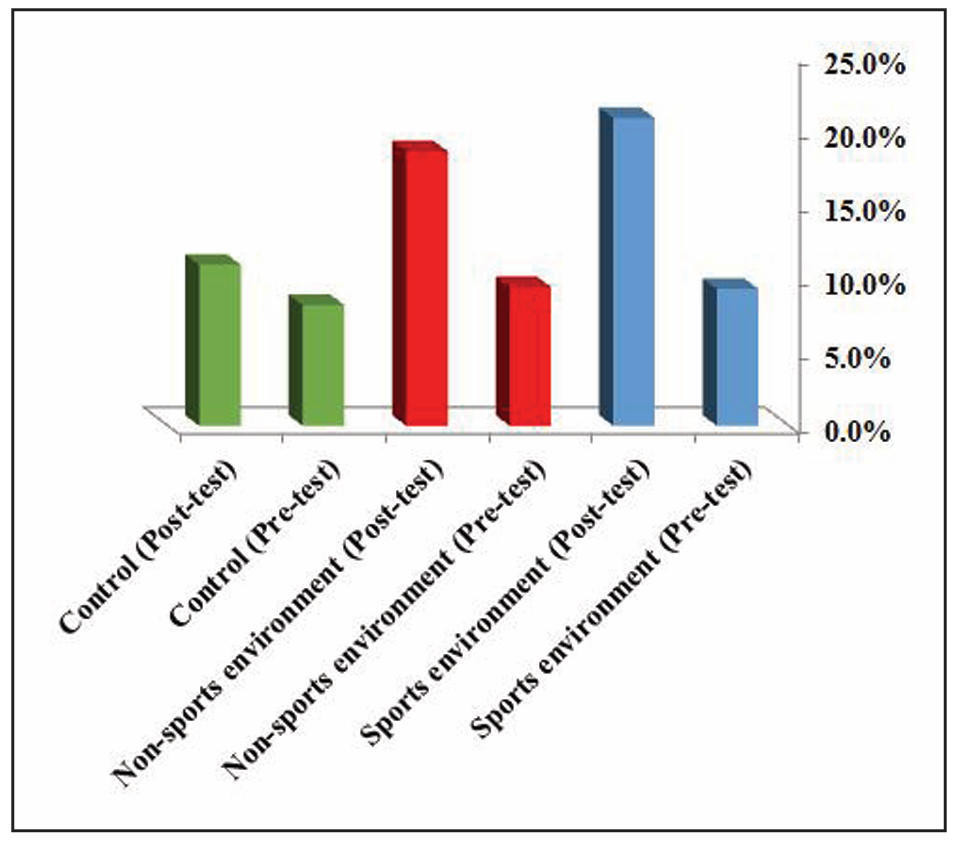
Figure 2. Results of groups' means based on optimism in the pre-test and post-test.
Next, to investigate the role of reminiscence therapy in sports and non-sports environments
on cognitive empowerment and optimism in the participants, a multivariate analysis of the
covariance (MANCOVA) was used. The use of this test requires compliance with statistical
assumptions such as: 1) normality of data distribution; 2) homogeneity of variance between
groups; 3) the observations are independent of one another, there is not any pattern for
the selection of the sample, and that the sample is completely random; 4) the independent
variables are categorical and the dependent variables are continuous or scale variables;
and 5) absence of multicollinearity i.e. the dependent variables cannot be too correlated
to each other [63]. Also, the Kolmogorov-Smirnov test was used to examine the normality of
data distribution, and the results showed that the distribution of cognitive
empowerment (Z = 1.28, sig = 0.15), and optimism (Z = 1.76, sig = 0.411) in the group of
reminiscence in a sports environment, and the distribution of cognitive empowerment
(Z = 1.66, sig = 0.253), and optimism (Z = 1.17, sig = 0.12) in the group of reminiscence
in a non-sports environment, was normal. Based on the results of Box’s M test, which was not
significant for any of the variables, the condition of homogeneity of the variance/covariance
matrices was properly met. The results showed that the variance/covariance matrices were
homogeneous (P = 0.22 > 0.05, F = 1.36, Box’s M = 17.53). Based on the results of Levene's
test, the variance of the scores of the reminiscence group in the sports environment in the
post-test for the cognitive empowerment (F1.426 = 0.345) and optimism (F1.211 = 0.296) and
the variance of the scores of the reminiscence group in the non-sports environment in the
post-test for the cognitive empowerment (F1.512 = 0.345) and optimism (F1.318 = 0.296) were
significant in both variables, considering that the significance level is greater than 0.05.
Therefore, it can be said that the variance of the variables in the post-test is homogeneous.
Also, the results of the Wilk's lambda showed that the effect of group on cognitive
empowerment and optimism is significant (P < 0.001, F = 18.20, Wilk's lambda = 0.118). The
above test allows the use of multivariate analysis of the covariance (MANCOVA). According to
the results of the regression homogeneity test, since the calculated F for the interaction
between the group and pre-test is not significant at a level less than 0.05, the data support
the regression homogeneity assumption.
The findings presented in Table 2 show that after removing the pre-test effect, there is
a significant difference between the three groups in all the above indicators. It should be
noted that considering the average correlation coefficients between the variables of this
hypothesis, all variables were analyzed in this hypothesis.
Table 2.
Multivariate analyses of covariance statistics.
| Test | Value | F | df | Sig. |
|---|---|---|---|---|
| Pillais trace | 1.25 | 17.49 | 33 | 0.01 |
| Wilk's lambda | 0.26 | 32.98 | 33 | 0.01 |
| Hotelling's trace | 10.46 | 58.26 | 33 | 0.01 |
| Roy's largest root | 11.66 | 122.46 | 33 | 0.01 |
Note F = Fischer; df = Degree of freedom; Sig. or P -value = *P < 0.05.
The findings presented in Table 2 show that after removing the pre-test effect,
there is a significant difference between the three groups in all the above indicators.
It should be noted that considering the average correlation coefficients between the
variables of this hypothesis, all variables were analyzed in this hypothesis.
Next, to investigate the role of reminiscence-based therapy in sports and non-sports
environments on cognitive empowerment and optimism in the participants, a multivariate
analysis of covariance (MANCOVA) test was used, the results of which are shown
in Table 3.
Table 3.
Examples of proteolytic enzymes involved in aging, along with their roles.
| Dependent variable | Source | Sum of squares | df | Mean of squares | F | Sig. | Eta coefficient |
|---|---|---|---|---|---|---|---|
| Cognitive empowerment | Pre-test | 234.35 | 1 | 234.35 | 214.80 | 0.059 | 0.76 |
| Group | 1702.12 | 2 | 715.16 | 519.81 | 0.001 | ||
| Optimism | Pre-test | 351.22 | 1 | 351.22 | 47.13 | 0.36 | 0.73 |
| Group | 1627.19 | 2 | 637.55 | 191.14 | 0.001 |
Note F = Fischer; df = Degree of freedom; Sig. or P-value = *P < 0.05.
As can be seen in Table 3, assuming control for pre-test effects, reminiscence-based interventions in sports and non-sports environments improved cognitive empowerment and optimism in the participants (P < 0.001). The results show that there is a significant difference between the two experimental and a control groups regarding cognitive empowerment and optimism, and the experimental groups are more effective than the control group. However, to accurately determine the difference between groups and compare the means pairwise, the Bonferroni post hoc test was used, the results of which are presented in Table 4.
Table 4.
Least significant difference test between the three groups in cognitive empowerment and optimism.
| Groups | Compared to the group | Variable | MD | Sig. |
|---|---|---|---|---|
| Reminiscence (sports environment) | Reminiscence (non-sports environment) | Cognitive empowerment | 4.4 | 0.000 |
| Optimism | 2.26 | 0.001 | ||
| Control | Cognitive empowerment | 26.14 | 0.001 | |
| Optimism | 9.91 | 0.000 | ||
| Reminiscence (non-sports environment) | Control | Cognitive empowerment | 21.74 | 0.001 |
| Optimism | 7.65 | 0.001 |
Note F = Fischer; df = Degree of freedom; Sig. or P-value = *P < 0.05.
As can be seen in Table 4, there is a significant difference between the three groups in the cognitive empowerment and optimism at the level of (P < 0.001). The results indicate that there is a significant difference between the indicators of the experimental groups (reminiscence in sports environment and reminiscence in non-sports environment) and the control group. Therefore, according to the aforementioned findings, it can be said that reminiscence in sports environment and reminiscence in non-sports environment improved and promoted indicators (cognitive empowerment and optimism) in the participants, and the intervention based on reminiscence in sports environment had a more effective role than reminiscence in non-sports environment.
Discussion
The study aimed to investigate the effect of structured group reminiscence in
sports and non-sports environments on cognitive empowerment and optimism in older
adults. Based on the findings, it was determined that reminiscence training in
sports and non-sports environments affects the cognitive empowerment of older adults.
This finding is consistent with the results of Musavi et al. [11], Khezri et al. [12],
Figar et al. [13], DeCoster and George [14], and Tarighat et al. [62], all of which
examined empowerment in the older adults and pointed out its importance. However,
no study was found that directly examined the effect of reminiscence intervention
on individuals' empowerment.
In this regard, successful intervention designs must also pay attention to understanding
the socio-cultural perspectives and characteristics of the population under study.
In this perspective, the participant is an active agent in the empowerment process,
and interventions emphasize less on changing behavior and more on bringing human potential
to a desirable and appropriate state. The empowerment process is dependent on the social
environment and is a social process that is achieved with the participation of others.
Therefore, as it was determined, the reminiscence intervention in the present study,
in both sports and non-sports environments, led to the improvement and increase of
cognitive empowerment of the participants and caused these individuals to improve
and enhance in eight areas of physical ability, self-esteem, spirituality, commitment,
role performance, situational awareness, self-management, and self-assessment through
the use of this intervention and the tools used.
Thus, it can be said that this intervention made the participants aware of changes in
memory and thinking, changes in sleep, irritability and feelings of anger, causes of
incontinence and urinary frequency, symptoms of the onset of Alzheimer's disease,
physical and mental problems resulting from retirement, a proper diet to protect
the body against diseases, efforts to achieve a sense of peace in their living
environment, appropriate decision-making in dealing with problems and ambiguous
life situations, efforts to maintain relationships with their loved ones, improving
patience in sensitive life situations, setting goals for the rest of their lives,
prioritizing those goals and trying to achieve them, and improving financial
management and spending in their lives, and other such things, and made them become
more capable and independent people in life, which in turn can improve life satisfaction
and increase life expectancy in these people.
The findings also showed that reminiscence training in sports and non-sports environments
resulted in improving optimism in older adults. This finding is consistent with the
results of Majzoubi et al. [39], Saleh Manige et al. [66], Kae-Hwa and Gyeong-Ju [67],
Boojari et al. [68], Sheykhi et al. [69], Ren et al. [70], and Sales et al. [71].
Majzoubi et al. showed that structured reminiscence interventions can significantly
increase the happiness of older adults and promote positive emotions in this
group [39]. Saleh Manige et al. stated that the presence of optimism in older adults
can lead to better perceptions of aging [66]. Also, Kae-Hwa and Gyeong-Ju suggest that
the use of a group reminiscence program can positively affect the life satisfaction
of older adults living in nursing homes as an effective intervention [67].
Boojari et al. also state that structured group reminiscence therapy can improve
psychological aspects of the quality of life of older adults [68].
Sheykhi et al. concluded that reminiscence can improve happiness and vitality in
retired older adults [69]. Ren et al. also stated that group reminiscence intervention
combined with exercise and physical activity led to the development and improvement
of spiritual well-being in older adults [70]. Also, Sales et al. stated that the
reminiscence program can improve the meaning of life, sense of coherence, and coping
strategies in older women living in nursing homes [71].
Therefore, according to the findings of the study and the results of other studies,
it can be observed that, in general, structured reminiscence intervention can lead to
the improvement and development of positive characteristics such as happiness and vitality,
life satisfaction, life expectancy, and the reduction of negative characteristics such as
death anxiety, depression, stress, etc., and ultimately, increase the level of optimism
towards life in older adults. Using the structured group reminiscence in the present
study resulted in the participants improving and upgrading their expectations for the
best in uncertain situations, being optimistic about the future, and expecting good
things to always happen to them. They also improved in areas such as expecting bad
things to happen to them, expecting things to usually go according to their wishes,
having low expectations for good things to happen to them, and being less pessimistic
about the rest of their lives.
Finally, the findings showed that reminiscence intervention in a sports environment
played a more effective role in increasing cognitive empowerment and optimism in older
adults compared to non-sports environments. This finding is consistent with the results
of studies by Ludwig et al. [50] Diez Roux and Mair [52], Ross and Mirowsky [57], Beard
et al. [60], Fannon [72] and Craig et al. [73], which have pointed out and confirmed
the effect of the environment on improving or impairing the psychological characteristics
of individuals.
Ludwig et al. suggested that living in a better neighborhood leads to long-term
improvements in adult physical and mental health and subjective well-being [50].
Diez Roux and Mair stated that features of neighborhoods or residential environments
may affect health and contribute to social inequalities in health [52]. Ross and Mirowsky
found that residents of disadvantaged neighborhoods have worse health (worse self-reported
health and physical functioning and more chronic conditions) than residents of more
advantaged neighborhoods and it is not mediated by limitation of outdoor physical activity.
The daily stress associated with living in a neighborhood where incivility is common, damages
health [57]. Beard et al. stated that an older adult's neighborhood of residence is an
important determinant of his or her mental health. Those making efforts to improve mental
health among the elderly need to consider the role of residential context in improving or
impairing mental health [60]. Fannon by comparing exercise environment and its effect on
changes in mood: indoors vs. outdoors, stated that only the feelings of elatedness and
energized were significantly shown to be more enhanced by exercising in a green outdoor
environment [72]. Craig et al. by exploring the effect of the environment on physical
activity, stated that the environment was positively associated with physical activity [73].
Limitations and recommendations for future studies
Among the limitations of the present study are the problems related to holding sessions due to the COVID-19 conditions, especially for the non-sports environment group who were in a closed environment, the occurrence of stress caused by COVID-19 and its interference with the variables under study, the lack of awareness of the mental and psychological conditions of the individuals when completing the questionnaires and during the program implementation, as well as individual and psychological differences and other disruptive factors that could cause deviations in the findings. We recruited participants who chose to be a volunteer for this program, so these people already have a positive attitude towards intervention, which could influence the results. Unfortunately, we could not report whether the experimental group's improvements would be maintained over time. Also, the sample size was rather small, although we conducted calculations and focused on effect size in the interpretation of the results. It is suggested that further research, the financial situation, and the level of education of the older adults should be additionally investigated, which can be among the components that affect the cognitive empowerment and optimism of the different populations.
Conclusions
The study concluded that both structured group reminiscence in sports and non-sports environments improves cognitive empowerment and optimism in older adults, Also reminiscence intervention in a sports environment played a more effective role compared to non-sports environments. Hence it can be said that structured group reminiscence in both environments can be used to train and achieve desired effect on specific components of psychological characteristics of older adults.
Declarations
Acknowledgements
We would like to express our gratitude to all the participants who helped us conduct this study.
Author contributions
All authors equally contributed to preparing this article.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
None.
References
1. United Nations, Department of Economic and Social Affairs. World population ageing 2020: highlights. from https://www.un.org/development/desa/pd/sites/www.un.org.development.desa.pd/files/2020/Sep/un_pop_2020_pf_ageing_10_key_messages.pdf.
2. Khazaei M, Marszałek J, Aminzadeh R, Dehghani E, & Azizi B. Benefits of Pilates exercises on functional fitness and quality of life in older men: a quasi-experimental study. Baltic Journal of Health and Physical Activity, 2024, 16(1): 3-13. [Crossref]
3. Mobaraki N, Esfahani M, Azimkhani A, & Azizi B. Investigating the relationship between quality of life and adherence to physical activity with life expectancy at leisure time in the elderly. Avrasya Spor Bilimleri ve Eğitim Dergisi, 2022, 4(1): 56-66. [Crossref]
4. Ramadan Abdel-Aziz H, & AbdElkhalek A. The effect of group reminiscence therapy on self-esteem and emotional well-being of older adults. Central European Journal of Nursing and Midwifery, 2021, 12(4): 513-520. [Crossref]
5. Shropshire M. Reminiscence intervention for community-dwelling older adults without dementia: a literature review. Br J Community Nurs, 2020, 25(1): 40-44. [Crossref]
6. Mendoza-Núñez V, Martínez-Maldonado Mde L, & Correa-Muñoz E. Implementation of an active aging model in Mexico for prevention and control of chronic diseases in the elderly. BMC Geriatr, 2009, 9: 40-51. [Crossref]
7. de la Luz Martínez-Maldonado M, Correa-Muñoz E, & Mendoza-Núñez V. Program of active aging in a rural Mexican community: a qualitative approach. BMC Public Health, 2007, 7: 276-286. [Crossref]
8. Santos S, Barlem E, Silva B, Cestari M, & Lunardi V. Health promotion for the elderly: gerontogeriatric nursing commitment. Acta Paulista de Enfermagem, 2008, 21: 649-653. [Crossref]
9. Vahedian-Azimi A, Alhani F, Goharimogaddam K, Madani S, Naderi A, & Hajiesmaeili M. Effect of family-centered empowerment model on the quality of life in patients with myocardial infarction: a clinical trial study. J Nurs Edu, 2015, 4(1): 8-22.
10. Ravanipour M, Salehi S, Taleghani F, & Abedi H. Power in old age: a qualitative study. Iranian journal of psychiatry and clinical psychology, 2009.
11. Musavi S, Ravanipour M, Pouladi S, Motamed N, & Barekat M. Evaluation of elderly cardiac patient's ability to receiving their needed social support. Iranian Journal of Rehabilitation Research, 2015, 1(3): 1-12.
12. Khezri R, Ravanipour M, Motamed N, & Vahedparast H. Effect of self-management empowering model on the quality of life in the elderly patients with hypertension. Iranian Journal of Ageing, 2016, 10(4): 68-79.
13. Figar S, Galarza C, Petrlik E, Hornstein L, Rodríguez Loria G, Waisman G, et al. Effect of education on blood pressure control in elderly persons: a randomized controlled trial. Am J Hypertens, 2006, 19(7): 737-743. [Crossref]
14. DeCoster V, & and George L. An empowerment approach for elders living with diabetes: a pilot study of a community-based self-help group—the diabetes club. Educational Gerontology, 2005, 31(9): 699-713. [Crossref]
15. Ferguson S, & Goodwin A. Optimism and well-being in older adults: the mediating role of social support and perceived control. Int J Aging Hum Dev, 2010, 71(1): 43-68. [Crossref]
16. Seligman M, Steen T, Park N, & Peterson C. Positive psychology progress: empirical validation of interventions. Am Psychol, 2005, 60(5): 410-421. [Crossref]
17. Vacek K, Coyle L, & Vera E. Stress, self-esteem, hope, optimism, and well-being in urban, ethnic minority adolescents. J Multicultural Counseling & Dev, 2010, 38(2): 99-111. [Crossref]
18. Carver C, & Scheier M. Dispositional optimism. Trends Cogn Sci, 2014, 18(6): 293-299. [Crossref]
19. Durbin K, Barber S, Brown M, & Mather M. Optimism for the future in younger and older adults. J Gerontol B Psychol Sci Soc Sci, 2019, 74(4): 565-574. [Crossref]
20. Jones T, DeMore M, Cohen L, O'Connell C, & Jones D. Childhood healthcare experience, healthcare attitudes, and optimism as predictors of adolescents' healthcare behavior. J Clin Psychol Med Settings, 2008, 15(3): 234-240. [Crossref]
21. Scheier M, Carver C, & Bridges M. Optimism, pessimism, and psychological well-being. 2001. [Crossref]
22. Weber S, Puskar K, & Ren D. Relationships between depressive symptoms and perceived social support, self-esteem, & optimism in a sample of rural adolescents. Issues Ment Health Nurs, 2010, 31(9): 584-588. [Crossref]
23. Aspinwall L. The psychology of future-oriented thinking: from achievement to proactive coping, adaptation, and aging. Motivation and Emotion, 2005, 29(4): 203-235. [Crossref]
24. Giltay E, Kamphuis M, Kalmijn S, Zitman F, & Kromhout D. Dispositional optimism and the risk of cardiovascular death: the Zutphen elderly study. Arch Intern Med, 2006, 166(4): 431-436. [Crossref]
25. Woods B, Spector A, Jones C, Orrell M, & Davies S. Reminiscence therapy for dementia. Cochrane Database Syst Rev, 2005, (2): Cd001120. [Crossref]
26. Syed Elias S, Neville C, & Scott T. The effectiveness of group reminiscence therapy for loneliness, anxiety and depression in older adults in long-term care: a systematic review. Geriatr Nurs, 2015, 36(5): 372-380. [Crossref]
27. Tam W, Poon S, Mahendran R, Kua E, & Wu X. The effectiveness of reminiscence-based intervention on improving psychological well-being in cognitively intact older adults: a systematic review and meta-analysis. Int J Nurs Stud, 2021, 114: 103847. [Crossref]
28. Lai C, Igarashi A, Yu C, & Chin K. Does life story work improve psychosocial well-being for older adults in the community? A quasi-experimental study. BMC Geriatr, 2018, 18(1): 119. [Crossref]
29. Meléndez Moral J, B. F, Alicia S, & Mayordomo Rodríguez T. Effect of integrative reminiscence therapy on depression, well-being, integrity, self-esteem, and life satisfaction in older adults. J Positive Psychol, 2015, 10(3): 240-247. [Crossref]
30. Musavi M, Mohammadian S, & Mohammadinezhad B. The effect of group integrative reminiscence therapy on mental health among older women living in Iranian nursing homes. Nurs Open, 2017, 4(4): 303-309. [Crossref]
31. Tarugu J, Pavithra R, Vinothchandar S, Basu A, Chaudhuri S, & John K. Effectiveness of structured group reminiscence therapy in decreasing the feelings of loneliness, depressive symptoms and anxiety among inmates of a residential home for the elderly in Chittoor district. Int J Community Med Public Health, 2019, 6(2): 847-854. [Crossref]
32. Afshari A, Rezai R, & Dadras F. The effectiveness of structured reminiscence on anxiety and depression in the elderly. Aging Psychology, 2019, 5(3): 201-215. [Crossref]
33. Wu Y, Xu H, Sui X, Zeng T, Leng X, Li Y, et al. Effects of group reminiscence interventions on depressive symptoms and life satisfaction in older adults with intact cognition and mild cognitive impairment: a systematic review. Arch Gerontol Geriatr, 2023, 114: 105103. [Crossref]
34. Sezer B, Kolaç N, Köse M, Safa İ, & Öğüt D. Effect of group reminiscence therapy on the loneliness, depression and life satisfaction of the elderly in the nursing homes. 2022, 13(3): 394–399. [Crossref]
35. Xu L, Li S, Yan R, Ni Y, Wang Y, & Li Y. Effects of reminiscence therapy on psychological outcome among older adults without obvious cognitive impairment: a systematic review and meta-analysis. Front Psychiatry, 2023, 14: 1139700. [Crossref]
36. Liu Z, Yang F, Lou Y, Zhou W, & Tong F. The effectiveness of reminiscence therapy on alleviating depressive symptoms in older adults: a systematic review. Front Psychol, 2021, 12: 709853. [Crossref]
37. Noghani F, Navab E, & Mehran A. The effects of group reminiscence therapy on loneliness and spiritual well-being among residents of Kahrizak nursing home. Iranian J Nurs Res, 2018, 13(1): 47-56.
38. Sahragard F, Rezaei M, Izadi-Avanji F, Atoof F, & Ahmadishad M. The effect of group reminiscence therapy on insomnia in older adults: a randomized controlled clinical trial. J Res Dev Nurs & Midwifery, 2020, 17(1): 94-110. [Crossref]
39. Majzoobi M, Momeni K, Amani R, & Hojjat Khah M. The effectiveness of structured group reminiscence on the enhancement of the elderlt, life quality and happiness. 2012.
40. Amani R. The effectiveness of structured group reminiscence on the enhancement of elderly's positive self-concept. Aging Psychology, 2015, 1(1): 1-9.
41. Ching-Teng Y, Chia-Ju L, & Hsiu-Yueh L. Effects of structured group reminiscence therapy on the life satisfaction of institutionalized older adults in Taiwan. Soc Work Health Care, 2018, 57(8): 674-687. [Crossref]
42. Zhong Q, Chen C, & Chen S. Effectiveness on quality of life and life satisfaction for older adults: a systematic review and meta-analysis of life review and reminiscence therapy across settings. Behav Sci, 2023, 13(10): 830-840. [Crossref]
43. Naveena J, Arora S, Srivastava S, & Vikas S. Structured reminiscence: an intervention to improve quality of life among older adults. Neuro Quantology, 2022, 20(9): 4691-4695. [Crossref]
44. Lodha P, & De Sousa A. Reminiscence therapy in geriatric mental health care: a clinical review. J Geriatr Mental Health, 2019, 6: 7-13. [Crossref]
45. Eryılmaz A, Yıldırım E, Kurtulus H, & Yıldırım M. Group reminiscence therapy interventions in non-clinical older adults: a systematic review. Geriatr Nurs, 2025, 63: 35-44. [Crossref]
46. Shortt N, Richardson E, Pearce J, & Mitchell R. Mortality inequalities by environment type in New Zealand. Health Place, 2012, 18(5): 1132-1136. [Crossref]
47. Nilsson K, Sangster M, Gallis C, Hartig T, de Vries S, Seeland K, et al. (2012). Forests, trees and human health. Springer.
48. Croezen S, Picavet H, Haveman-Nies A, Verschuren W, de Groot L, & van't Veer P. Do positive or negative experiences of social support relate to current and future health? Results from the Doetinchem Cohort Study. BMC Public Health, 2012, 12: 65-75. [Crossref]
49. Zunzunegui M, Alvarado B, Del Ser T, & Otero A. Social networks, social integration, and social engagement determine cognitive decline in community-dwelling Spanish older adults. J Gerontol B Psychol Sci Soc Sci, 2003, 58(2): S93-s100. [Crossref]
50. Ludwig J, Duncan G, Gennetian L, Katz L, Kessler R, Kling J, et al. Neighborhood effects on the long-term well-being of low-income adults. Science, 2012, 337(6101): 1505-1510. [Crossref]
51. Chetty R, Hendren N, & Katz L. The effects of exposure to better neighborhoods on children: new evidence from the moving to opportunity experiment. Am Econ Rev, 2016, 106(4): 855-902. [Crossref]
52. Diez Roux A, & Mair C. Neighborhoods and health. Ann NY Acad Sci, 2010, 1186: 125-145. [Crossref]
53. Robert SA. Socioeconomic position and health: the independent contribution of community socioeconomic context. Annual Review of Sociology, 1999, 25: 489-516. [Crossref]
54. Leventhal T, & Brooks-Gunn J. The neighborhoods they live in: the effects of neighborhood residence on child and adolescent outcomes. Psychol Bull, 2000, 126(2): 309-337. [Crossref]
55. Aminzadeh R, Khazaei M, Dzioban K, Azizi B, & Elham D. Quality of life and adherence to physical activity in leisure time of people with physical disability. Biomedical Human Kinetics, 2024, 16: 41-48. [Crossref]
56. Browning C, Cagney K, & Boettner B (2016). Neighborhood, place, and the life course. Handbook of the Life Course: Volume II. M. J. Shanahan, J. T. Mortimer and M. Kirkpatrick Johnson. Springer, Cham: 597-620.
57. Ross C, & Mirowsky J. Neighborhood disadvantage, disorder, and health. J Health Soc Behav, 2001, 42(3): 258-276.
58. Almedom A. Social capital and mental health: an interdisciplinary review of primary evidence. Soc Sci Med, 2005, 61(5): 943-964. [Crossref]
59. Whitley E, Gunnell D, Dorling D, & Smith G. Ecological study of social fragmentation, poverty, and suicide. Bmj, 1999, 319(7216): 1034-1037. [Crossref]
60. Beard J, Cerdá M, Blaney S, Ahern J, Vlahov D, & Galea S. Neighborhood characteristics and change in depressive symptoms among older residents of New York city. Am J Public Health, 2009, 99(7): 1308-1314. [Crossref]
61. Anderson C. (2024). What is regular physical exercise? from https://focuskeeper.co/glossary/what-is-regular-physical-exercise
62. Tarighat M, Ravanipour M, Pouladi S, & N. M. Design and psychometric analysis of the cognitive ability questionnaire of the elderly about individual changes. Iranian South med J, 2017, 20(2): 193-206. [Crossref]
63. Scheier M, & Carver C. Optimism, coping, and health: assessment and implications of generalized outcome expectancies. Health Psychol, 1985, 4(3): 219-247. [Crossref]
64. Carver C, & Scheier M (2001). Optimism, pessimism, and self-regulation. Optimism & pessimism: implications for theory, research, and practice. Washington, DC, US, American Psychological Association: 31-51.
65. Stinson C. Structured group reminiscence: an intervention for older adults. J Contin Educ Nurs, 2009, 40(11): 521-528. [Crossref]
66. Manige H, Papi S, Sahaf R, Asl M, Ramshini M, Rassafiani M, et al. Predicting the perception of aging based on optimism in the elderly people. Iranian J Ageing, 2020, 14(4): 450-461. [Crossref]
67. Kae-Hwa J, & Gyeong-Ju A. Effects of a group reminiscence program on self-forgiveness, life satisfaction, and death anxiety among institutionalized older adults. Korean J Adult Nurs, 2018, 30(5): 546-557. [Crossref]
68. Boojari S, Niazi J, Talezadeh Shirazi R, & S. G. Effect of group reminiscence therapy on quality of life in older adults in shiraz city. Scientific J Rehabilitation Med, 2019, 7(4):110890. [Crossref]
69. Sheykhi A, Navidian A, Keykha R, & Nasrin R. Effect of reminiscence on the happiness the retired elderly members of the islamic republic of Iran army. IJN, 2019, 32(119): 1-12. [Crossref]
70. Ren Y, Tang R, Sun H, & Li X. Intervention effect of group reminiscence therapy in combination with physical exercise in improving spiritual well-being of the elderly. Iran J Public Health, 2021, 50(3): 531-539. [Crossref]
71. Sales A, Pinazo-Hernandis S, & Martinez D. Effects of a reminiscence program on meaning of life, sense of coherence and coping in older women living in nursing homes during COVID-19. Healthcare, 2022, 10(2): 188-198. [Crossref]
72. Fannon C. Study of exercise environment and its effect on changes in mood: indoors vs. outdoors. Southern Illinois University-Carbondale, 2015.
73. Craig C, Brownson R, Cragg S, & Dunn A. Exploring the effect of the environment on physical activity: a study examining walking to work. Am J Prev Med, 2002, 23(2 Suppl): 36-43. [Crossref]
Supplementary
Table Appendix A.
Structured group reminiscence program
| Session | Session's Topic | Session's stimulus | Session's target |
|---|---|---|---|
| 1 | Preparations | Birth certificate, marriage certificate, and anything that identifies the person | Making people feel comfortable, introducing people to each other, starting reminiscence, creating interest and enthusiasm in people, and remembering the people who played a role in naming them |
| 2 | Childhood and family life | Family photos, childhood games, jump ropes, marbles, and all the toys of that time | Creating a sense of belonging to the group, reliving the feeling of childhood, working together to remember the past |
| 3 | School life | Blackboard, chalk, school bag, school reports, pen, educational globe, school uniform, teacher's name, school location | Continuing to build a sense of belonging to the group, re-experiencing the good and bad aspects of school life, recreating the feelings prevalent during that time |
| 4 | Starting a career and working life | Work tools, wooden ruler, old money, educational certificate, work apron | Appreciating one's past skills and achievements, finding memories and common ground among group members, describing the joys of youth |
| 5 | Going outdoors and having fun | Open environment, green space, special tourist places in the city | Remembering past pleasures, the feeling of youth, beauty, and good looks, sharing experiences, such as going to the movies, the first romantic relationship, the first perfume used, etc. |
| 6 | Marriage | Marriage certificate, wedding ring, wedding photos, wedding gift, love letters, engagement period | Remembering the things they did to maintain their marital relationship, paying attention to and remembering the most beautiful moments in life and sharing shared experiences |
| 7 | Home, garden, and pets | Paintbrush and bucket, gardening tools, hammer, old houses, photos of old neighborhoods | Recalling the home environment in which they lived during childhood, adolescence, youth, marriage, and adulthood, recalling related activities and skills, and the individual's home ( e.g., gardening, home decoration design) |
| 8 | Next generation, infants and toddlers | Old baby bottle, large safety pin, baby bib, doll, baby oil, baby care book, baby naming book, knitting patterns, baby clothes, photos of babies in old clothes | Recalling the time they took care of their baby or child and the memories related to it, the child's smile and emotions, their noises and movements, tickling and following them, kissing them and their mischief |
| 9 | Food and cooking | Cookbooks, wooden spoons and mixing bowls, tea trays, photos of various foods | Recalling important discoveries in the field of cooking, providing an opportunity to remember and apply past skills, collaborating with others to do cooking |
| 10 | Vacations and travel | Souvenirs, travel luggage, backpacks, maps, vehicles, shells, mementos of each city | Reminiscing about the richness of people's lives and their past accomplishments and adventures, sharing current passions and favorite places, and reminiscing about the joys and misfortunes that have befallen them on trips and vacations |
| 11 | Celebrations | Most of the stimuli for this session were provided by families | Creating an opportunity for participants to be together and celebrate togetherness, and acknowledging the people who participated in the sessions |
| 12 | Summarizing sessions | Photos of the project, writings and drawings, and activities of individuals, displaying the family diary in the project | Hearing from everyone about what these sessions meant to them, remembering what group members have accomplished during these days and planning for future sessions |