Open Access | Research article
This work is licensed under a Creative Commons Attribution-ShareAlike 4.0 International License.
Effect of dual task training versus analogy training on gait speed and balance in older adults—randomized controlled trial
* Corresponding author: Reema Joshi
Mailing address: Department of General and Community based rehabilitation, Dr. D.Y. Patil College of Physiotherapy, Pimpri, Pune, India.
E-mail: yashi2000shah@gmail.com
Received: 14 October 2024 / Revised: 02 November 2024 / Accepted: 11 November 2024 / Published: 28 March 2025
DOI: 10.31491/APT.2025.03.167
Abstract
Background: Walking performance is often impaired by both cognitive and motor tasks, especially in the elderly. These tasks result in reduced speed, longer strides, and increased variability in stride length. Cognitive methods, including attentional tactics, self-instruction strategies, or external cues, can improve gait. This study aims to determine the effect of dual training and analogy training on gait speed and balance in older adults.
Methods: This three-arm, parallel, single-blind, randomized control trial was conducted, 116 participants were screened out of which 69 individuals (aged 60-75 years) were allocated into 3 groups with the allocation ratio of (1:1:1), group A dual task training, group B analogy training, group C control group. Training sessions lasted 45 min, 3 days per week for 4 weeks. For assessment, the time up and go test, modified fall efficacy scale, activity specific balance confidence scale, 10-meter walk test and Tinetti performance-oriented mobility assessment scale were performed before and after.
Results: The Mann-Whitney U test was used to determine the difference between groups, and the Wilcoxon sign rank test was used for within-group analysis. Time up and go test shows significant improvement in group A (P = 0.02). The 10-meter walk test shows significant improvement in preferred walking speed, maximum walking speed, and activity confidence in group B (P = 0.0001).
Conclusion: This study concludes that analogy training was superior to dual-task training and the control group and can be used as an effective mode of gait rehabilitation to improve gait speed and balance in the elderly. Analogy training and dual-task training can be used for gait rehabilitation in older adults.
Keywords
Analogy training, dual-task training, gait rehabilitation, geriatric, walking speed and balance
Introduction
According to the World Health Organization (WHO), healthy aging is the process of acquiring and maintaining the functional abilities necessary for well-being in old age [1]. Effective aging, with less cognitive decline and comparatively greater well-being, is made possible by the reorganization of brain networks [1]. The global prevalence of falls was 26.5%, with Oceania—which includes nations such as Australia, New Guinea, Papua, Samoa and others—having the highest prevalence at 34.4%. According to the 2011 census, 104 million Indians are over the age of 60, or about 8.6% of the population [2]. Fall risk factors associated with healthy aging include intrinsic factors such as loss of skeletal muscle mass, muscle fiber atrophy resulting in a decrease in muscle cross-sectional area, neuromuscular changes such as motor neuron loss, and axonal nerve conduction velocities that slow with age. Reduced terminal sprouting can lead to a decreased process of re-innervation of muscle fibers, reducing motor unit recruitment. Extrinsic factors such as lighting, flooring, and furniture can create obstacles to walking and lead to falls [3]. As age progresses, it also affects cognition and the domains of cognition, which are orientation, attention, memory, communication, and executive function. Working memory, processing speed, attention span, executive control, and episodic memory can all be affected by aging. This can lead to deficits in working memory and processing speed. This can also affect an older adult's gait. Age-related impairments in neuromuscular, sensory, and cognitive abilities complicate the complex task of walking. Executive function can be described as task performance, which includes memory, and cognitive planning, which includes active problem solving and working memory. Evidence from Andre Mojitola et al. suggests that executive function capacity declines with age, as assessed by inhibition, shifting, and dual-tasking in young adults [4-6]. Cognitive-motor and motor dual activities are essential in daily life. However, previous studies have shown that attempting to balance two tasks simultaneously can negatively affect gait. Studies also show that when older adults with a history of pain and cognitive impairment are unable to perform cognitive-motor tasks, single-task exercises with minimal cognitive demands can improve speed and balance. The practice of teaching specific concepts through multiple iterations of task-specific exercises to improve task performance is a fundamental principle of motor learning and can be incorporated in healthy individuals. It has been suggested that single-task training may not be as effective as dual-task training in improving dual-task performance in healthy older adults. When introducing a new topic and providing background information about it, analogy may occur. According to Zhu, Poolton, and Wilson Hu, et al., analogy learning makes information processing easier and more efficient, but it can also lead to a decrease in verbal-cognitive regulation of movement. In traditional learning formats, practice sometimes requires the conscious application of explicit instructions or guidelines, which can be neither easy nor effective [7, 8]. After receiving analog training, Parkinson's patients improved their walking ability. These benefits were seen in dual-task cognitive (counting backwards) and motor (carrying a tray) scenarios, in addition to a simple walking test. Melanie Kleynen's study found that analog training also significantly changed stride speed, stride height and stride width in stroke patients [9]. Both cognitive and motor demands affect gait performance, resulting in slower gait, longer strides, and greater stride length variability, especially in the elderly population. This can lead to reduced functional mobility and quality of life, falls, and low self-esteem. Cognitive techniques such as attentional tactics (self-generated with an internal focus), self-instructional strategies, or external cues (visual, tactile, or auditory) can help improve gait. The combination of cognitive and physical learning approaches can improve working memory, processing speed, and multitasking ability. In order to develop effective therapeutic interventions for future fall prevention programs, it is essential to investigate the potential effects of dual-task analogy training on rehabilitation outcomes. Therefore, the purpose of this study was to determine how dual-task analogy training affects gait speed and balance in older adults.
Methods
Study design: Randomized controlled trial.
Study setting: This study was conducted in Dr. D.Y. Patil College of Physiotherapy, Pimpri, Pune between September 2023 and January 2024.
Study population: The population for this study is older adults between the age of 60-75 years old.
Sampling method: purposive sampling.
The inclusion criteria were:
1. Both male and female will be included
2. Subject above 60-75 years, Montreal cognition assessment with 26-30 for normal cognition
3. Tinetti’s performance-oriented mobility assessment scale (POMA) score higher than 19 out of 28
4. Time up and go test score less than 20 sec
The exclusion criteria were:
1. Neurological impairments
2. Recent fractures
3. Visual impairments which cannot be corrected by glass
4. Vestibular impairment
5. Use of assistive device (cane, walker)
6. Cognitive impairments
7. Presence of artificial prosthesis
Data collection
The sample size was calculated by estimating the
prevalence rate. Given that the prevalence of falls
in older adults was 23%, an acceptable difference
of 10% with a 95% confidence interval, and a power
of 80%, the sample size was calculated to be 69 (23 in each group).
Ethical approval was obtained from the Institutional
Review Board number DYCPT/ IEC/37/2023. The Clinical
Trial Registration India (CTRI) number was CTRI/2023/05/053338.
Subjects were screened, screened and enrolled with written
informed consent and informed subject explanation
form in their respective languages.
Data collection procedure and instrumentation
The 116 subjects were screened and 69 participants who met the inclusion and exclusion criteria were enrolled in the study (Figure 1). The purpose, benefits, and nature of the study were explained to the participants. Written and verbal informed consent was obtained from all participants prior to enrollment. Based on the inclusion and exclusion criteria, participants were randomly divided into 3 groups with an allocation ratio of (1:1:1) by computerized randomization: group A-dual task training, group Banalogy training, and group C-control group based on exclusion and inclusion criteria.
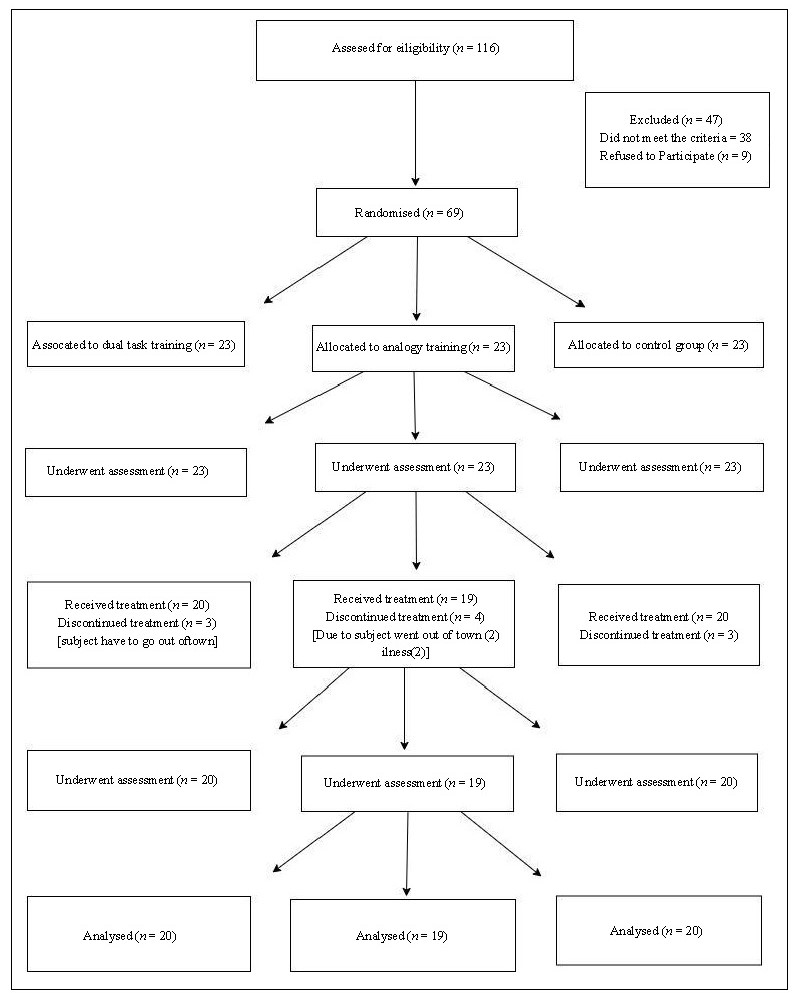
Figure 1. Consort chart.
Treatment protocol
The intervention lasted 4 weeks in total (Table 1 and Table 2). During this time, participants were trained in the order of their group: dual-task training, analogy training, control group. In the first two weeks, Group A and Group B, the protocol was for a duration of 40 minutes with 10 minutes of warm up, 20 minutes of walking protocol with subsequent breaks followed by 10 minutes of cool down. Group A and B participants were supervised throughout the sessions to ensure safety. Group C was asked to continue with their daily walking routine. Sessions were stopped at any time during the procedure, taking into account the termination criteria. Assessment was done per-intervention and post-intervention.
Table 1.
Dual task training 4 week (Total session - 12 sessions).
| Sessions | Protocol | Illustration | |
|---|---|---|---|
| 1st week | 3 sessions/week | Walk with counting backwards. |
|
| 2nd week | 3 sessions/week | Walk with counting backwards, obstacles walking, speed alterations. |
|
| 3rd week | 3 sessions/week | Walk with counting backwards, zig-zag patterns, speed alteration. |
|
| 4th week | 3 sessions/week Walk | Walk with counting backwards, figure of 8 patterns, speed alteration. |
|
Table 2.
Analogy training 4 week (total session—12 sessions).
| Sessions | Protocol | Illustration | |
|---|---|---|---|
| 1st week | 3 sessions/week | Walk as if you follow foot prints. |
|
| 2nd week | 3 sessions/week | Try to cross a small bridge. |
|
| 3rd week | 3 sessions/week | Walk as if you are crossing the signal on road. |
|
| 4th week | 3 sessions/week | Walk imagining you are kicking a football in front of you |
|
Walking speed is assessed using the 10-meter walk test, balance and mobility using Tinetti's Performance Oriented Mobility Assessment (POMA) scale, dynamic balance using the timed up & go test, fear of falling using the Modified Fall Efficacy Scale, and confidence in performing the activity using the Activity Specific Balance Confidence Scale.
Statistical analysis
Data were analyzed using the SPSS 26.0 statistical package (SPSS Inc., Chicago, IL, USA), and the significance level was set at P < 0.05. Descriptive statistics were used to evaluate the mean and standard deviation of each group. Normality of the data was assessed using the Shapiro-Wilkinson test. Inferential statistics to determine within-group differences were performed using the Kruskal-Wallis test followed by the Bonferroni post hoc test. Between-group analysis was performed using the MannWhitney U test. The chi-squared test was used to analyze differences in proportions.
Results
Statistical software SPSS 26.0 (SPSS Inc., Chicago, IL, USA) was used to analyze the data, with a significance threshold of P < 0.05. Descriptive statistics were used to evaluate the mean and standard deviation of each group. Nonparametric tests are used for the study because Table 3 shows the mean deviation of baseline data for age, sex, height, weight, BMI, and MOCA score. The ShapiroWilkinson test for normality showed a significant difference (P < 0.05) between the mean and standard deviation of age.
Table 3.
Baseline demographic data.
| Characteristics | Dual task (mean ± SD) | Analogy training (mean ± SD) | Control group (mean ± SD) | P value |
|---|---|---|---|---|
| Age, years | 63.75 ± 3.768 | 64.89 ± 4.829 | 63.45 ± 0.857 | 0.50 |
| Gender |
Male, 8 Female, 12 |
Male, 11 Female, 8 |
Male, 10 Female, 10 |
0.06 |
| Height, cm | 156.10 ± 6.091 | 155 ± 5.470 | 158.20 ± 7.082 | 0.24 |
| Weight, kg | 64.51 ± 5.332 | 63.14 ± 4.423 | 63.67 ± 6.957 | 0.73 |
| BMI, kg/m2 | 26.49 ± 2.058 | 26.37 ± 2.528 | 25.50 ± 3.125 | 0.11 |
| MoCA | 28.90 ± 0.850 | 28.95 ± 0.911 | 29.10 ± 0.852 | 0.61 |
Note: Table 3 shows the mean with standard deviation of age, gender, height, weight, BMI, MOCA in dual task (group A), analogy training (group B), control group (group C).
The mean and standard deviation of the pre and post timed up and go test scores for each of the three groups are shown in Table 4. Nonparametric tests are used for analysis because the Shapiro-Wilkinson test for normality showed a significant difference (P < 0.05). For 'TUG', the between-group analysis showed statistically significant differences for both pre- and post-intervals (P < 0.05). Bonferroni post hoc test showed a significant difference between all pairwise groups except Dual task vs. Analogy (P > 0.05) in the 'Pre' interval. According to the withingroup analysis, there was a significant decrease (P < 0.05) in Analogy and dual task between Pre and Post. Dual task > Analogy > Control (highest to lowest) is the observed mean difference (Pre-Post).
Table 4.
Pre and post mean and SD of outcome measures with statistical analysis.
| Time up and go test | Pre (Second) | Post (Second) | Mann Whitney U test | P value | Mean difference |
|---|---|---|---|---|---|
| Group A | 14.41 ± 3.34 | 11.47 ± 3.61 | 2.45 | 0.001* | 2.94 ± 3.47 |
| Group B | 12.69 ± 2.22 | 11.41 ± 1.57 | 2.10 | 0.04* | 1.28 ± 1.89 |
| Group C | 9.61 ± 1.11 | 9.39 ± 1.05 | 0.64 | 0.52 (N.S.) | 0.22 ± 1.08 |
| P value (Kruskal Wallis test) |
0.0001* |
0.0001* | |||
| P value (Bonferroni post hoc test) |
A vs. B A vs. C B vs. C |
0.06 0.0001* 0.0004* |
0.02* 0.0001* 0.02* |
||
| Poma | Pre | Post | Independent test | P value | Mean difference |
| Group A | 25.85 ± 1.77 | 26.5 ± 1.36 | 1.30 | 0.20 (N.S.) | 0.65 ± 1.56 |
| Group B | 26.37 ± 1.26 | 27.05 ± 0.89 | 1.97 | 0.05* | 0.68 ± 1.01 |
| Group C | 27.3 ± 1.01 | 27.3 ± 1.01 | 0.01 | 0.99 (N.S.) | 0 ± 1.01 |
| P value (Kruskal Wallis test) | 0.005* | 0.07 | |||
| P value (Bonferroni post hoc test) |
A vs. B A vs. C B vs. C |
0.46 0.004* 0.09 |
0.26 0.06 0.75 |
Note: *P < 0.05 is statistically significant. N.S., Not significant.
The data in Table 5 did not follow a normal distribution. Therefore, the analysis was performed using non-parametric tests. For "preferred walking", a statistically significant difference was found between the groups for both the pre- and post-intervals (P < 0.05). A 10-meter walk test was used to compare walking speeds between and within groups. The mean and standard deviation of the pre and post values for all three groups are shown. The normality test, Shapiro-Wilkinson, showed a significant difference (P < 0.05), so the analysis was performed using non-parametric tests. The Kruskal-Wallis test for between-group analysis showed a statistically significant difference for "preferred walking" for both pre- and post-intervals (P < 0.05). The Mann-Whitney U test for within-group analysis showed a significant difference (P < 0.05) between Pre and Post for the analogy group only. The observed mean difference (Pre-Post) is shown below: Analogy > Dual task = Control (highest to lowest).
Table 5.
Pre and post comparison of preferred walking speed and ‘maximum walking speed’.
| 10-meter walk test (maximum walking speed) | Pre | Post | Mann Whitney U test | P value | Mean difference |
|---|---|---|---|---|---|
| Group A | 0.92 ± 0.10 | 0.98 ± 0.13 | 1.63 | 0.11 (N.S.) | 0.06 ± 0.11 |
| Group B | 1.02 ± 0.13 | 1.22 ± 0.21 | 3.62 | 0.0009* | 0.2 ± 0.17 |
| Group C | 1.03 ± 0.16 | 1.07 ± 0.16 | 0.79 | 0.43 (N.S.) | 0.04 ± 0.16 |
| P Value (Kruskal Wallis test) | 0.01* | 0.0002* | |||
| P value (Bonferroni post hoc test) |
A vs. B 0.05 A vs. C 0.02* B vs. C 0.96 |
0.0001* 0.22* 0.01* |
|||
| 10-meter walk test (preferred walking speed | Pre | Post | Independent test | P value | Mean difference |
| Group A | 0.82 ± 0.08 | 0.81 ± 0.08 | 0.39 | 0.69 (N.S.) | 0.01 ± 0.08 |
| Group B | 0.87 ± 0.10 | 1.07 ± 0.21 | 3.84 | 0.0004* | 1.94 ± 0.15 |
| Group C | 0.92 ± 0.13 | 0.93 ± 0.13 | 0.24 | 0.80 (N.S.) | 0.01 ± 0.13 |
| P value (Kruskal Wallis test) | 0.01* | 0.0001* | |||
| P value (Bonferroni post hoc test) |
A vs. B 0.29 A vs. C 0.01* B vs. C 0.29 |
0.0001* 0.03* 0.01* |
Note: * P < 0.05 is statistically significant. N.S., not significant.
The results of the between and within group analyses for the Activity-Specific Balance Confidence Scale are shown in Table 6. A significant difference (P < 0.05) was found using the Shapiro-Wilkinson normality test. Therefore, the tests are nonparametric. A statistically significant difference (P < 0.05) was found for both the Pre and Post periods according to the Kruskal-Wallis test for betweengroup analysis. With the exception of Dual task vs. Analogy and Analogy vs. Control (P > 0.05) in the Pre interval and Dual Task vs. Control in the Post interval, the Bonferroni post hoc test revealed a significant difference between all pairwise groups. Only the Analogy group showed a significant difference between Pre and Post (P < 0.05) when analyzed within groups using the Mann-Whitney U test. The mean difference (Pre-Post) was as follows: Analogy > Dual task > Control (highest to lowest).
Table 6.
Pre and post comparison of comparisons activity—specific balance confidence scale.
| Pre | Post | Independent T test | P value | Mean difference | |
|---|---|---|---|---|---|
| Group A | 0.78 ± 0.05 | 0.80 ± 0.06 | 1.14 | 0.25 | 0.02 ± 0.05 |
| Group B | 0.83 ± 0.06 | 0.86 ± 0.05 | 1.71 | 0.09 | 0.03 ± 0.05 |
| Group C | 0.82 ± 0.04 | 0.82 ± 0.04 | 0.01 | 0.99 | 0 ± 0.04 |
| P value (Kruskal Wallis test) | 0.006* | 0.001* | |||
| P value (Bonferroni post hoc test) |
A vs. B 0.007* A vs. C 0.04* B vs. C 0.80 |
0.001* 0.43 0.04* |
Note: *P < 0.05 is statistically significant.
Discussion
We investigated the effects of dual-task and analogy
training on balance and gait speed in older adults. Participants
reported 34% of falls in the dual task training (DT) group,
21.7% in the analogy group (AG), and 26% in the control
group.
The TUG time for each participant in the dual-task training was less than 13.5 seconds, indicating a lower risk
of falling. It is possible that the TUG increased during
dual-task training because they already had more time
to complete the test, and dual-tasking has been shown to
affect frontal lobe activation, which can increase
cognitive load in older people [10]. Dual-task
training tests the somatosensory system by
transmitting postural information from muscle
and joint proprioceptors to the primary
somatosensory brain. This sensation provides information
about the relative orientation and movement of the body
in relation to the supporting surface [11]. The vestibular
system is very sensitive to angular and linear acceleration
of head position, which is also a challenge during the dual
task of zig-zag and figure-8 pattern walking. The visual
stimulation required to overcome obstacles during
walking has also helped to improve postural stability during
gait. Marcelo, Paula, and Pamala et al. suggest that
dualtask training helps to improve static and dynamic balance
in older adults [11].
Dual-task training uses focal vision to locate the visual
stimulus, while analogy training focuses on the surround
vision in which the unconscious stimulus was used. Research
by Kitchana and Phongphat et al. found that an
audio-visual cue affected walking speed in both healthy
older adults and those with balance problems. The findings
suggest that audio-visual cues can be used to encourage
healthy lifestyle choices in older people with balance
problems [12, 13].
Preferred walking and maximal walking were found to
be significantly improved by analogy training because it
reduces cognitive demands during training. Experiments
have shown that explicit motor learning (dual-task training)
can impair walking performance, which can lead to
limiting walking speed and hindering walking activity. In
this study, they also found that counting numbers backwards
decreased walking speed.
The Activity Specific Balance Confidence Scale is a
structured questionnaire that measures an individual's
confidence in performing ambulatory activities without falling.
In this study, the ABC scale was found to be significantly
improved by analogy training over dual-task training.
Subjects reported a significant increase in confidence after
analogy training because analogy training involved
everyday environmental stimuli. The use of familiar analogies
in gait rehabilitation helps to reduce working memory
while walking, which leads to improved confidence and
reduced risk of falling while walking. These goals can be
achieved by using analogy in gait rehabilitation and improving subjects' confidence.
In this study, Tinetti's POMA scale was used to assess
stability and balance. Therefore, the statistical analysis
shows statistically significant results within the AG than
DT and control group. However, there was no statistical
significance between the three groups. The POMA scale
assesses both mobility and balance in subjects in this
study; the population included had good balance and mobility.
The control group was advised to perform a daily
walking routine at home, and it was found that the control
group showed no significant changes compared to the
analogy training and dual-task training.
Both types of training are inexpensive and easy to implement
in the physical therapy setting. Dual-task training can be
used with older subjects at lower risk of falling,
while analogy training can be used with subjects at high
risk of falling. The initial phase of gait training, where
training can begin with less working memory and these
challenges can be progressively increased, also helps to
improve confidence in the early stages, then more challenging
dual-task training can be planned to improve the
cognitive-motor dual-task with training that focuses on
a targeted specific task with a cognitive task. Dual-task
training and analogy training can also be used as a preventive
training strategy in geriatric rehabilitation to prevent
older adults from losing their balance and to improve gait.
This study had the following limitations. First, the duration
of the study was limited. Second, the protocol for
both dual-task training and analogy training was delivered
by the same instructor. Third, health outcomes were not
assessed beyond 30 days after the sessions. Finally, the
small sample size may limit the generalizability of our
findings to other populations. Therefore, long-term studies
should be conducted to determine the effect of this training,
two different trainers should implement the protocol
for the dual-task and analogy training groups, and a large
sample size should be used.
Conclusions
This study concludes that analogy training was superior to dual-task training and the control group and can be used as an effective form of gait rehabilitation to improve gait speed and balance in older adults.
Declarations
Acknowledgment
The authors would like to thank the Institution for supporting us in this research article.
Author contributions
CT and YS wrote the research article under the supervision of RJ. RJ is a professor with a specialization in general and community-based rehabilitation. All the authors contributed to the final manuscript.
Conflicts of interest
All authors declare that they have no competing interests.
Financial support and sponsorship
This study received no specific grant from any funding agency in the public commercial or not-for-profit sector.
Data availability
All data generated or analyzed during the present study are available from the corresponding author upon reasonable request.
Ethical approval and informed consent
The Ethical approval was obtained from the Institutional review board with the number DYPCPT/IEC/37/2023. Clinical Trial Registration India (CTRI) was done with the number CTRI/2023/05/053338.
References
1. Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, & Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas, 2020, 139: 6-11. [Crossref]
2. The longitudinal ageing study in India 2017-18 - national report, international institute for population sciences, national programme for health care of elderly, ministry of health and family welfare, Harvard T. H. Chan School of Public Health, and the University of Southern California, 2020.
3. A. G (2012). Geriatric physical therapy-2nd Edition.
4. Alenazi AM, Alanazi MF, Elnaggar RK, Alshehri MM, Alqahtani BA, Alhowimel AS, et al. Prevalence and risk factors for falls among community-dwelling adults in Riyadh area. Peer J, 2023, 11: e16478. [Crossref]
5. O'Sullivan SB, Schmitz TJ, & Fulk GD (2014). Physical Rehabilitation, 6th edition.
6. Abdallat R, Sharouf F, Button K, & Al-Amri M. Dual-task effects on performance of gait and balance in people with knee pain: a systematic scoping review. J Clin Med, 2020, 9(5): 1554-1564. [Crossref]
7. Glynn SM (1994). Teaching science with analogies a strategy for teachers and textbook authors.
8. Gentner D. Structure-mapping: a theoretical framework for analogy. Cognitive Science, 1983, 7(2): 155-170. [Crossref]
9. Jie LJ, Goodwin VA, Kleynen M, Braun S, Nunns M, & Wilson MR. Analogy learning in Parkinson's disease: a proof-of-concept study. Int J Therapy Rehabilitation, 2016, 23: 123-130.
10. Mirelman A, Maidan I, Bernad-Elazari H, Nieuwhof F, Reelick M, Giladi N, et al. Increased frontal brain activation during walking while dual tasking: an fNIRS study in healthy young adults. J Neuroeng Rehabil, 2014, 11: 85-96. [Crossref]
11. Nascimento MM, Maduro PA, Rios PMB, Nascimento LDS, Silva CN, Kliegel M, et al. The effects of 12-week dual-task physical-cognitive training on gait, balance, lower extremity muscle strength, and cognition in older adult women: a randomized study. Int J Environ Res Public Health, 2023, 20(8): 5498-5503. [Crossref]
12. Kaewkaen K, Wongsamud P, Ngaothanyaphat J, Supawarapong P, Uthama S, Ruengsirarak W, et al. The influence of audio-visual cueing (traffic light) on dual task walking in healthy older adults and older adults with balance impairments. Malays J Med Sci, 2018, 25(1): 67-74. [Crossref]
13. Magnani PE, Zanellato NFG, Genovez MB, Alvarenga IC, Faganello-Navega FR, & de Abreu DCC. Usual and dual-task gait adaptations under visual stimulation in older adults at different ages. Aging Clin Exp Res, 2022, 34(2): 383-389. [Crossref]