Open Access | Research
This work is licensed under a Creative
Commons Attribution-ShareAlike 4.0 International License.
Effect of Pilates versus resistance training on physical fitness in older adults
* Corresponding author: Manisha Ashish Rathi
Mailing address: Khyati College of Physiotherapy, Ahmedabad, Gujarat, India. Khyati Dr. D. Y. Patil College of Physiotherapy,
Dr. D. Y. Patil Vidyapeeth, Pimpri, Pune, Maharashtra, India.
Email: manisharathi2405@gmail.com
Received: 27 July 2024 / Revised: 15 August 2024 / Accepted: 06 September 2024 / Published: 30 September 2024
DOI: 10.31491/APT.2024.09.149
Abstract
Background: Aging causes decline in various systems leading to affect physical fitness. It is necessary to implement new ways to improve physical fitness. Pilates training (PT) increases muscular control, strength and flexibility and resistance training (RT) works on strength and endurance. But how it affects in the older people is unclear. Hence the objective of this study was to compare the effect of Pilates and resistance training on physical fitness in older adults.
Materials and methods: This experimental study was conducted on 47 participants who participated into two groups: PT (n = 23) and RT (n = 24). Both training was given for 3 times/week for 6 weeks. Outcome measures were body composition (body fat, body weight, and body mass index), Strength (pushup test, squat test), flexibility (sit and reach test, shoulder and wrist elevation test), muscle endurance (one-minute sit to stand test) and cardiorespiratory endurance (six-minute walk test.) Level of significance was 95%.
Results: Within group analysis of PT and RT showed non-significant improvement in body composition (p < 0.05) but significant improvement in strength, muscle flexibility, muscle endurance (p > 0.01). PT showed significant difference in cardio-respiratory endurance (p = 0.02) whereas RT didn't show the same (p = 0.23). When both groups were compared, PT showed more improvement in flexibility and cardio-respiratory endurance (p < 0.05) whereas RT showed significantly better improvement in muscle strength and muscle endurance (p < 0.05).
Conclusion: The study concluded that both Pilates and resistance training can be used to improve physical fitness depending on the desired effect needed to improve specific components of physical fitness.
Keywords
Pilates, resistance training, older adults, physical fitness
Introduction
Aging is a decline and deterioration in functional properties at the cellular, tissue and organ level. This declination in
functional properties produces the loss of homeostasis and decreases the adaptability to internal and external stress finally leading
to an increased vulnerability to diseases and mortality [1]. Functionality can be defined as
having the ability to carry out daily tasks safely, independently, and without becoming exhausted
[2]. Reduction in strength and aerobic capacity in personal are greatly associated with
declines in functional ability of that individual, and this ultimately results in decreased levels of independence
[3]. In every country, the number of older people and their share of the population is rising.
By 2030, one in six people will be 60 or above. By 2050, there will be 1.4 billion people over the age of 60, up from 1 billion in
2020. India has seen an increase in this share, going from 5.6% in 1961 to 10.1% in 2021 and by 2031, which is projected to 13.1%
[4]. In India, more than one-third older people are obese, making them particularly vulnerable
to negative outcomes since obesity exacerbates the age-related decline in physical function and makes them weaker
[5].
The rise of various complex health conditions known as geriatric syndromes is feature of older age. They include weakness, stumbles,
urine incontinence, delirium and pressure ulcers which are frequently the result of numerous underlying conditions
[6]. Muscle strength gradually declines from the age of 50 and further declines by 12% to 15%
per ten years beyond that. Obesity is another factor of ageing. Energy expenditure during rest and during activity decreases with age.
Compared to resting energy expenditure, the decline is more pronounced in activityrelated energy expenditure. With increased adiposity
and visceral fat distribution, these metabolic changes are expected to raise the risk of dyslipidemia, insulin resistance, and
cardiovascular disease in older people. Sarcopenia plays a role in the development of osteopenia and its progression to osteoporosis,
as well as the relationship between muscles mass, strength and bone mineral density in older persons
[7].
The aged should adopt exercise regimens centered on four physical fitness components (cardiorespiratory endurance, muscle strength,
flexibility, and body composition) according to guidelines on fundamental exercises. Physical fitness has a direct impact on functional
independence in older persons. Physical activity (PA) is regarded as one of the most significant health markers since it improves
older persons more than any other major age group. Benefits of PA for individuals in this age may include increase in physical fitness
and prevention of functional loss. Long periods of inactivity can be broken up with brief bursts of activity, usually of a light
intensity, which may be advantageous for a number of brain-related processes. These include blood pressure, vascular function,
coagulation, sympathetic activity, and metabolism of carbohydrates and lipids. Breaking up extended sitting may also have acute
benefits and reduce fatigue, increase cerebral blood flow velocity, and improve cognitive performance
[8].
Resistance training (RT) encourages the muscles to contract against an external resistance in the intention of enhancing strength,
power, hypertrophy, and/or endurance [9]. Dumbbells, exercise tubing, your own body weight,
blocks, water bottles, or any other object that makes the muscles contract can be used as external resistance. In older individuals,
resistance training provides a powerful stimulus for skeletal muscle growth and increasing strength
[10]. Resistance training exercise program mainly focuses on center of the body which results
in positive effects on static and dynamic balance and improves the isokinetic strength of the knee
[11].
The Pilates method, a fitness regimen created by Joseph Pilates in 20th century, has been used as a kind of physical activity to
increase muscular control, strength, and flexibility, especially in the lumbar and pelvic regions, which are crucial for daily tasks.
Six fundamental concepts serve as the foundation for the Pilates method: force, concentration, control, accuracy, flow of movement, and
breathing [12]. Pilates has the ability to sync movement with breathing, also increases
overall body fitness and enhances one's ability to move and carry out daily tasks. It is crucial for senior citizens to keep their
independence [13]. Pilates practice tends to be effective in reducing obesity by improved
body composition, functional physical fitness, and basal metabolic rate in community-dwelling middleaged women
[14, 15]. The Pilates training (PT) program was
more effective for improving isometric hip and trunk extension strength, while the Muscular training program generated greater benefits
on trunk and hip isokinetic strength. Moreover, both training programs showed moderate effects for the TUG
[16].
However, there is lack of information concerning the effectiveness of these two types of training on all the components of physical
fitness, and the relationship between these variables has not yet been analyzed in older adults. Also, no studies have compared the
effectiveness of both interventions. Hence the aim of the study is to compare the effects of Pilates vs. Resistance training on
physical fitness in older adults.
Materials and methods
This experimental study was conducted at Dr. D. Y. Patil College of Physiotherapy, Pimpri, Pune from September 2022 to January 2023. This study was approved by Institutional Ethics Committee of Dr D.Y. Patil College of Physiotherapy, Pune with the Reference number DYPCPT/IEC/14/2022 and this was registered under Clinical Trial Registry of India (CTRI) with registration number is CTRI/2022/09/045134 dated 1st September 2022. Sample size was 47. It was calculated considering the prevalence of decreased level of fitness in older patients of 7%, acceptable difference of 5% at 95% confidence interval, power at 80%. After screening the participants, they were finally recruited and then divided randomly by using computer sequence generator into 2 groups, PT and RT, 25 participants in each group but there were 3 drop outs, so finally 47 participants completed the study, 24 in PT group and 23 in RT group (Figure 1).
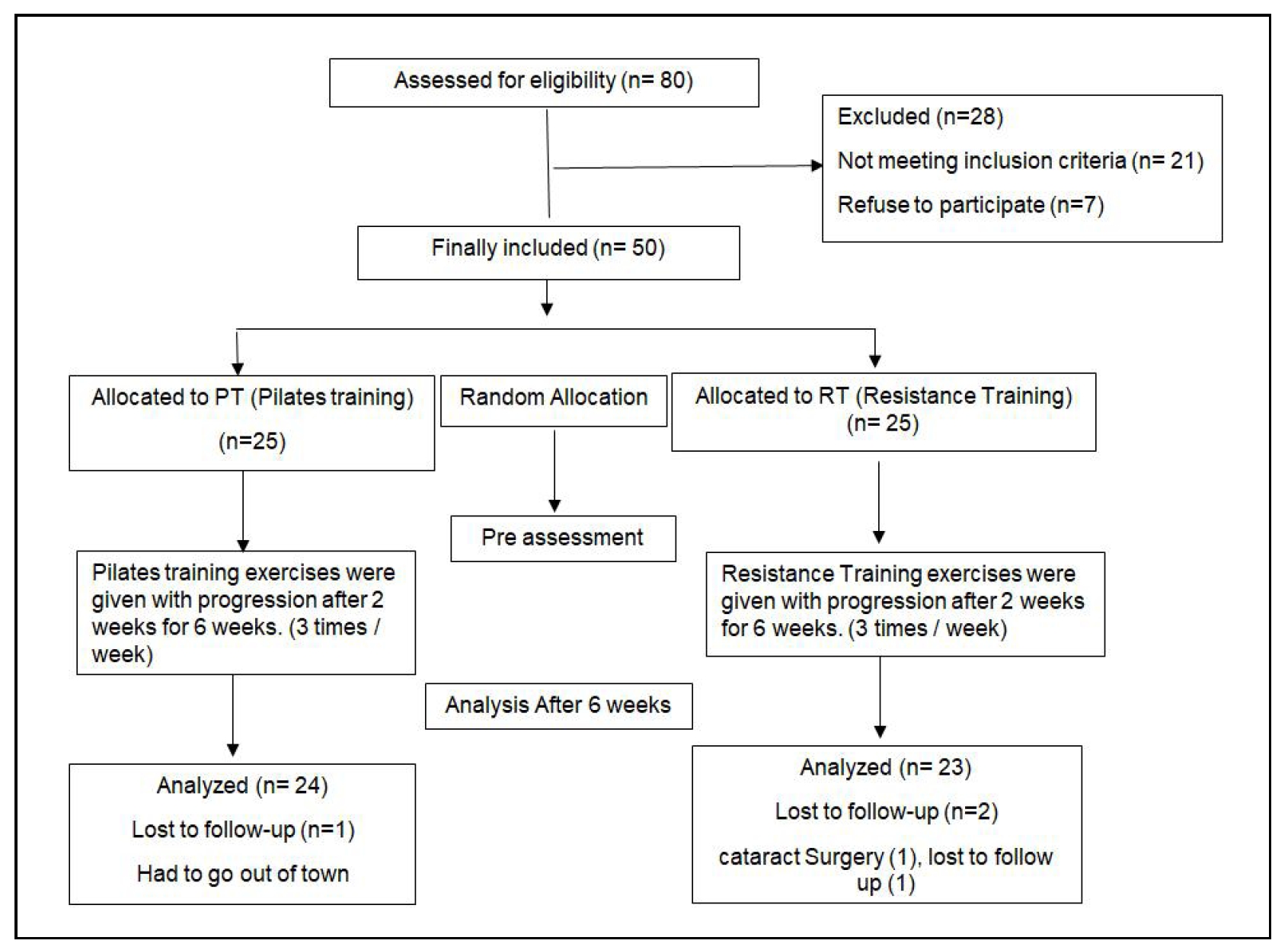
Figure 1. Consort chart.
The inclusion criteria were:
1. Adults from 60-75 years of age
2. No current involvement in any form of physical exercise or experience of Pilates
3. Body mass index (BMI): above 25 and up to 30 (25-30)
4. Initial Fitness criteria: VO2 max of 26-29 mL/kg/min for older men and VO2 max of 28-31 mL/kg/min for older women
The exclusion criteria were:
1. Any recent history of traumatic injury for 6 months
2. Any Serious illness (Cardiac, neurological and musculoskeletal disorders; psychological disorders) affecting implementing exercise
protocol
3. History of drug or alcohol abuse
4. Uncontrolled Diabetes mellitus (DM) or Hypertension (DM: 180 mL/dL or higher, systolic blood pressure ≥ 140 mmHg and diastolic blood
pressure ≥ 90 mmHg).
5. Exercise induced or uncontrolled angina within 3 months, or severe dyspnea at rest
6. Visual or auditory impairment not corrected with glasses or a hearing aid
Participant from both PT and RT groups performed exercise for 45 minutes, 3 days/week for 6 weeks. Each session consisted of 5 min warm
up, 30 min exercise and 5 min cool down. Exercise capacity of each individual was assessed initially as per inclusion criterion and the
participant was accompanied by the physiotherapist throughout the protocol to ensure safety.
Procedure
After ethical permission, various old age homes and nongovernmental organizations were approached and permission was obtained prior
to the study. Explanation of the study was given to the participants. On the basis of inclusion and exclusion criteria, participants
were included and written informed consent was taken from all the participants. Demographic details were taken and then assessed for
the baseline outcome measures.
The tests were stopped anytime during the procedure keeping in mind the termination criteria [If the participant chooses to stop
anytime during the test, Tachycardiaabove predicted HRmax (HRmax = 220-Age), Systolic BP more than 200 mmHg and diastolic BP more than
120 mmHg, palpitations, excessive paleness, excessive diaphoresis, muscle cramps and fatigue, dizziness/syncope, intolerable dyspnea.
Details of PT and RT protocol are given in Table 1 and
Table 2 respectively. All these exercises were given for 3 sets of 10 repetitions each.
Table 1
Pilates training (PT) protocol of 6 weeks.
| Week 1 & 2 | Week 3 & 4 | Week 5 & 6 | |
|---|---|---|---|
| Warm up | Diaphragmatic breathing Posterolateral breathing Neutral series Toe tap Abs prep Bridging Knee sway Abs prep |
Diaphragmatic breathing Posterolateral breathing Neutral series Toe tap Abs prep Bridging Heel slides Single leg raise |
Diaphragmatic breathing Posterolateral breathing Neutral series Toe tap Abs prep Bridging Heel slides Single leg raise |
| Exercises | Half roll down 100 Roll up Leg circle Single leg stretch Swimming Single leg kick Side leg kick Quadruped hip extension Half push-ups |
Bicycle crunches Hot potato Shoulder bridge Rowing Push-ups Swan dive Mountain climbers Fire hydrants Leg kicks Swimming |
Swan dive Abs with knee extended Plank Push-ups 100 (advance) Hot potato Boomerang Shoulder bridge Mountain climbers Prone hip extension |
| Cool-down | Stretching of hamstring, adductors, hip flexors. Waist oblique, child pose |
Stretching of hamstring, adductors, hip flexors. Waist oblique, child pose |
Stretching of hamstring, adductors, hip flexors. Waist oblique, child pose |
Table 2
Resistance training (RT) protocol of 6 weeks.
| Week 1 & 2 (using body weight) | Week 3 & 4 (Dumbbells/Thera band) | Week 5 & 6 (Dumbbells/Thera band) | |
|---|---|---|---|
| Warm up | Neck side bends Shoulder shrugs Arm rotations Wrist rotations Step up and down Marching |
Neck side bends Shoulder shrugs Arm rotations Wrist rotations Step up and down Marching |
Neck side bends Shoulder shrugs Arm rotations Wrist rotations Step up and down Marching |
| Exercises | Squats Wall push-ups Toe stands Half push-ups Forward lunges Side lunges Step down Pike push-ups Prone on elbows |
Biceps curls Triceps Overhead press Side hip raise Knee curls Floor back extension Squats Forward lunges Side lunges |
Biceps curls Triceps Overhead press Side hip raise Push-ups Pike push-ups Squats Forward lunges Side lunges |
| Cool-down | Stretching of hamstring, adductors, trapezius hip flexors. Waist oblique, child pose |
Stretching of hamstring, adductors, trapezius hip flexors. Waist oblique, child pose |
Stretching of hamstring, adductors, trapezius hip flexors. Waist oblique, child pose |
Outcome measure
a) Body composition
• Weight (kg) and Body fat percentage (%) was measured using Body fat analyzer (Omron Karada Scan Body Composition Monitor HBF-375).
• BMI was then calculated as per the formula: weight in kg/(height in meter)2 (Height was measured using stadiometer in meters).
b) Flexibility
• Sit and reach test assesses flexibility of low back and hamstrings. Fix a meter stick on top of the box such that 26 cm of the ruler
protrudes towards the test participant over the front edge. The box's edge should be at the 26 cm mark. The patient is seated with their
legs straightened out and parallel to the floor's marked tape line. The heels of the feet should be about 10 to 12 inches apart and touch
the edge of the box. As far as possible, the patient should slowly stretch his or her arms forward and place one hand on top of the other
with the palms facing down. Mark the reading at the end point [17].
• Shoulder and wrist elevation test was used for upper extremity flexibility. Participant has to lay face down on the ground with his arms
outstretched and hands grasping an 18" stick shoulder-width apart. The participant is then raising the stick as high as participant can
while keeping the forehead on the ground, then measures the vertical distance from the ground to the bottom of the stick.
c) Muscle strength
• Pushup test was used for assessment of muscle strength of upper limb. For this, participant in prone position, keep back straight while
knee on the floor with hands on either side of the chest. Always bring chest down to the same level, until either elbows are at right
angles or chest touches the floor. Do as many pushups as possible until participant is completely exhausted. Make a sum of all the pushups
correctly performed for scoring [17].
• Squat test was used for assessment of muscle strength of lower limb. Place feet in front of the chair or bench at shoulder width apart,
hands placed on hips. Ask participant to squat, gently contact the chair, and then get back to standing. Do this repeatedly until
participants maximally can do [17].
d) Muscle endurance
• One-minute sit and stand test was used to assess muscle endurance. Keep the chair's back against a wall to prevent it from moving during
the test. Participants in a seated position with hands on hips and arms at sides and feet should be parallel to the ground. When
participants stand from the chair, wait until legs are completely straight then sit down. This is single sit-to-stand. Continue getting in
and out of the chair as frequently as you can do in one minute and total is considered as final reading
[17].
e) Cardio-respiratory endurance (CRE)
CRE was assessed using 6-minute walk test to calculate VO2 max. Participant is asked to walk for 6 minutes in a 30 m hallway at
a normal pace. Prior to the test and posttest HR, BP and SpO2 are measured. The patient is allowed to take pause if any
discomfort feels in between the test. The number of laps and distance walked is noted posttest. VO2 max is calculated with help
of test [18].
Statistical analysis
Data was analyzed using the statistical package SPSS 26.0 (IBM SPSS Inc., Chicago, IL) and level of significance was set at p < 0.05. Normality of the data was assessed using Shapiro Wilkinson test. Normally distributed data was analyzed by paired t test and t test whereas if the parameters were not normally distributed, data was analyzed using Mann Whitney U test and Wilcoxon sign rank test.
Results
Demographic characteristics (age, height) reported in Table 3 showed baseline data was matching. Female participants in this study were more than the male participants. The pre and post mean with standard deviation of outcome measures (Table 4) showed non-significant improvement in body composition (assessed by body weight, BMI and Body fat percentage) in both groups whereas changes in muscle strength (assessed by Pushup test and squat test), flexibility (assessed by wrist and shoulder elevation test), muscle endurance (assessed by sit and stand test) and cardiorespiratory endurance (assessed by 6 min walk test) showed significant improvement in both groups. Flexibility assessed by sit and reach test showed significant improvement with Pilates training but non-significant improvement with resistance training.
Table 3
Baseline characteristics of the data.
| Variables | Pilates Training (n = 25) | Resistance Training (n = 25) | p value |
|---|---|---|---|
| Age in years | 66.25 ± 3.77 | 67 ± 5.23 | 0.52 |
| Height in meters | 1.53 ± 0.06 | 1.55 ± 0.05 | 0.08 |
| Gender | |||
| Male | 0 | 2 | - |
| Female | 25 | 23 | - |
Table 4
Pre and post mean and SD of outcome measures with statistical analysis.
| Outcome measures | Pilates Training (n = 25) | Resistance Training (n = 25) | |||||
| Fitness component | Test performed | Pre | Post | p value | Pre | Post | p value |
| Body composition | Weight (kg) | 63 ± 7.81 | 60.8 ± 7.73 | 0.27 | 67 ± 6.01 | 64.44 ± 5.69 | 0.09 |
| BMI (kg/m2) | 26.99 ± 2.6 | 25.06 ± 2.61 | 0.87 | 27.81 ± 2.39 | 26.76 ± 2.32 | 0.90 | |
| Body fat percentage (%) | 32.18 ± 3.4 | 30.95 ± 3.41 | 0.17 | 34.81 ± 4.84 | 33.72 ± 4.81 | 0.71 | |
| Muscle strength | Pushup test no. on one min (n) | 26.17 ± 6.36 | 30.62 ± 6.71 | 0.01* | 26.32 ± 5.14 | 36.08 ± 5.02 | > 0.01** |
| Squat test no. on one min (n) | 30.41 ± 6.13 | 38.91 ± 6.38 | > 0.01** | 25.96 ± 3.82 | 35.8 ± 3.89 | > 0.01** | |
| Muscle flexibility | Sit and reach test (cm) | 4.29 ± 3.39 | 7.75 ± 3.32 | > 0.01** | 2.44 ± 3.82 | 4.12 ± 3.77 | 0.08 |
| Wrist and shoulder elevation test (cm) | 13.5 ± 3.12 | 16.5 ± 3.37 | 0.01* | 10.92 ± 2.48 | 12.72 ± 3.14 | 0.01* | |
| Muscle endurance | Sit and stand test (repetition/min) | 27.12 ± 4.04 | 36.75 ± 3.60 | > 0.01** | 25.28 ± 4.01 | 35.76 ± 4.69 | > 0.01** |
| Cardio-respiratory endurance | 6 min walk test VO2 max (mL/kg/6 min) | 26.48 ± 4.21 | 29.86 ± 4.19 | 0.02* | 27.72 ± 3.65 | 28.82 ± 3.54 | 0.23 |
Note: *Significant, **Highly significant.
When both groups were compared, analyses showed resistance training had significantly more improvement than Pilates training on muscle strength (assessed by Pushup test and squat test) and muscle endurance (assessed by sit and stand test). But muscle flexibility (assessed by sit and reach test and wrist and shoulder elevation test) and cardio-respiratory endurance (assessed by 6 min walk test) reported significantly better improvement in Pilates training than Resistance training (p > 0.05). Non-significant difference was observed in body composition assessed by body weight, BMI and body fat (%). Details are shown in Table 5.
Table 5
Mean difference of pre and post values of both the groups and statistical analysis.
| Outcome measures | Pilates Training (n = 25) | Resistance Training (n = 25) | p value | |||
| Fitness component | Test performed | Difference between pre and post mean | Effect Size | Difference between Pre and Post mean | Effect size | Body composition | Weight (kg) | 2.2 ± 1.46 | 0.25 | 2.56 ± 1.02 | 0.29 | 0.24 |
| BMI (kg/m2) | 1.93 ± 0.45 | 0.17 | 1.06 ± 0.41 | 0.20 | 0.23 | |
| Body fat percentage (%) | 1.23 ± 0.53 | 0.23 | 1.09 ± 0.35 | 0.19 | 0.21 | Muscle strength | Pushup test no. on one min (n) | 4.45 ± 2.08* | 0.39 | 9.76 ± 1.51 | 0.86 | > 0.001** |
| Squat test no. on one min (n) | 8.5 ± 2.43** | 0.66 | 9.84 ± 1.73 | 0.76 | 0.01* | Muscle flexibility | Sit and reach test (cm) | 3.45 ± 1.32** | 0.43 | 1.68 ± 0.73 | 0.21 | >0.001** |
| Wrist and shoulder elevation test (cm) | 3 ± 1.35* | 0.36 | 1.8 ± 2.01 | 0.21 | 0.006* | |
| Muscle endurance | Sit and stand test (repetition/min) |
9.63 ± 1.82** | 0.93 | 10.42 ± 2.01 | 0.82 | 0.02* |
| Cardio-respiratory endurance | 6 min walk test VO2 max (mL/kg/6 min) | 3.38 ± 2.15* | 0.29 | 1.09 ± 0.32 | 0.09 | >0.001** |
Note: *Significant, **Highly significant.
Discussion
The aim of this study was to compare the effects of Pilates and Resistance training on various components of physical fitness among
older adults. In this experimental study, 47 older adults were included and their mean age in PT was 66.25 ± 3.77 and in RT was 67 ± 5.23.
Many other studies didn't include older people or took individuals from 18 to 80 years old, which has become wide age span. As older
persons were more for developing the risk of numerous morbidities and cardiovascular diseases, this study recruited them to evaluate their
level of physical fitness.
This study showed non-significant difference in body composition assessed by weight, BMI and Body fat percentage. This was supported by
Taskiran and Markovic who reported no alteration in body composition following the PT but Fourie et al. reported that
percentage of fat mass decreased while the percentage of lean mass increased after PT [19,
20]. Although the duration of the two researches was comparable, it is challenging to compare
them because many studies gave information about the repetitions, progress of the workouts, and intensity. Taskiran and Markovic employed
bio-impedance while Fourie et al. used skinfold measurement to determine body composition, which may partially account for the
variations in results. The use of skinfolds in the elderly is controversial in the literature despite the fact that both techniques are
frequently utilized. This is because older people tend to have thicker, more elastic skin, and redistribute their subcutaneous fat
differently, which could affect the accuracy of procedure [21]. Effects of RT on older persons
found that concurrent rise in fat-free mass, little to no change in total body weight and decreases in fat mass. Hence RT has primary
impact on body composition by changing the ratio of fat to muscle mass. This is not the case with aerobic exercise where there has little
to no growth in fat-free mass but reduction in body fat and bodyweight due to its fat burning process
[22].
Muscle Strength was assessed using modified pushup test (upper limb) and squat test (lower limb) which was improved more in RT compared to
PT. According to the overload principle of strengthening, strength improves with RT. It is a powerful form of exercise for reversing
the age-related decline in muscular strength. For instance, after RT upper and lower body strength can dramatically improve, with
improvements ranging from 9 to 174%. Notably, RT increases muscle strength even in extremely old people (85 years of age)
[1].
Being flexibility as an important component of physical fitness, sit and reach test and shoulder & wrist elevation test reported
significant improvement in Pilates training. Pilates training adds dynamic stretching activities along with distinct muscle-strengthening
exercises for various body parts (legs, trunk and upper limbs). As this technique combines stretching and strengthening exercises in the
same session, it gives positive impact on flexibility. Resistance training for 16 weeks can increase joints ranges of motion and more
results was observed in last 8 weeks of training. Due to 6-week period of our study, Pilates demonstrated better gains in flexibility than
RT [23].
This study showed significant improvement in muscle endurance; more in RT than PT. This may be due to the increase in oxidative capacity,
larger mitochondrial concentrations and more powerful oxidative enzymes. There is also increase in capillary density through RT. It also
alters skeletal muscle morphology and can enhance tensile strength of elderly tendons thereby increasing muscle endurance
[24].
CRE plays an important role in geriatric fitness. This study showed more improvement in PT compared to RT. Beneficial effect of Pilates
training can be breathing exercises, ribcage flexibility exercises and lumbopelvic region strengthening was observed. First,
Pilates-induced lumbopelvic and core muscular development may result in more effective upper and lower limb movement patterns as well as
stronger expiratory muscles. Second, the increased flexibility may enable the ribcage to move with greater efficiency. Finally, the
breathing exercises may improve intercostal muscle functionality and lung capacity. Based on these principles, it would be possible to
improve ventilation efficiency, leading to a greater flow of oxygenated blood into muscle tissues, improved local circulation, increased
muscle oxidative capacity, and less energy waste. Hence PT could achieve CRE with minimal intensity
[25, 26].
The limitation in this study was follow up was not taken after 6 weeks and there were more female participants in the study than male and
the results calculated were not considered on the basis of gender. The future scope of the study is that more duration of intervention can
be given. The study can be gender specific and research can be done on community dwelling elders.
Conclusions
The study concluded that Pilates training improves flexibility and cardiorespiratory endurance significantly whereas resistance training showed significant improvement in muscle strength and muscle endurance. Hence both type of exercises can be used to train and achieve desired effect on specific components of physical fitness.
Acknowledgements
We thank Miss Anuprita Dixit for giving us permission to work with her Non-Governmental Organizations and all the participants of the study. We are thankful to the statistician who helped for analysis of the study.
Declarations
Author contributions
All authors equally contributed to preparing this article.
Availability of data and materials
Not applicable.
Financial support and sponsorship
None.
Conflicts of interest
None
Consent for publication
Not applicable.
References
1. Holliday R. Developmental and cell biology series. Understanding Aging, 1995, 30: 41-66.
2. Hunter GR, McCarthy JP, & Bamman MM. Effects of resistance training on older adults. Sports medicine, 2004, 34: 329-348. [Crossref]
3. Fleg JL, Morrell CH, Bos AG, Brant LJ, Talbot LA, Wright JG, et al. Accelerated longitudinal decline of aerobic capacity in healthy older adults. Circulation, 2005, 112(5): 674-682. [Crossref]
4. Rudnicka E, Napierała P, Podfigurna A, Męczekalski B, Smolarczyk R, & Grymowicz M. The World Health Organization (WHO) approach to healthy ageing. Maturitas, 2020, 139: 6-11. [Crossref]
5. Villareal DT, Chode S, Parimi N, Sinacore DR, Hilton T, Armamento-Villareal R, et al. Weight loss, exercise, or both and physical function in obese older adults. N Engl J Med, 2011, 364(13): 1218-1229. [Crossref]
6. Inouye SK, Studenski S, Tinetti ME, & Kuchel GA. Geriatric syndromes: clinical, research, and policy implications of a core geriatric concept. J Am Geriatr Soc, 2007, 55(5): 780-791. [Crossref]
7. Padilla Colón CJ, Molina-Vicenty IL, Frontera-Rodríguez M, García-Ferré A, Rivera BP, Cintrón-Vélez G, et al. Muscle and bone mass loss in the elderly population: advances in diagnosis and treatment. J Biomed (Syd), 2018, 3: 40-49. [Crossref]
8. Nehrkorn-Bailey AM, Rodriguez D, Forsyth G, Braun B, Burke K, & Diehl M. Change in views of aging, physical activity, and physical health over 8 weeks: results from a randomized study. J Aging Phys Act, 2023, 31(4): 666-678. [Crossref]
9. Moore DR, Burgomaster KA, Schofield LM, Gibala MJ, Sale DG, & Phillips SM. Neuromuscular adaptations in human muscle following low intensity resistance training with vascular occlusion. Eur J Appl Physiol, 2004, 92(4-5): 399-406. [Crossref]
10. Cannataro R, Cione E, Bonilla DA, Cerullo G, Angelini F, & D'Antona G. Strength training in elderly: an useful tool against sarcopenia. Front Sports Act Living, 2022, 4: 950949. [Crossref]
11. Marques EA, Mota J, Machado L, Sousa F, Coelho M, Moreira P, et al. Multicomponent training program with weight-bearing exercises elicits favorable bone density, muscle strength, and balance adaptations in older women. Calcif Tissue Int, 2011, 88(2): 117-129. [Crossref]
12. Bertoli J, Biduski GM, & de la Rocha Freitas C. Six weeks of Mat Pilates training are enough to improve functional capacity in elderly women. J Bodyw Mov Ther, 2017, 21(4): 1003-1008. [Crossref]
13. Fernández-Rodríguez R, Álvarez-Bueno C, Ferri-Morales A, Torres-Costoso A, Pozuelo-Carrascosa DP, & MartínezVizcaíno V. Pilates improves physical performance and decreases risk of falls in older adults: a systematic review and meta-analysis. Physiotherapy, 2021, 112: 163-177. [Crossref]
14. Pereira MJ, Dias G, Mendes R, Mendes RS, Martins F, Gomes R, et al. Efficacy of Pilates in functional body composition: a systematic review. Applied Sciences, 2022, 12(15): 7523. [Crossref]
15. Su CH, Peng HY, Tien CW, & Huang WC. Effects of a 12-week Pilates program on functional physical fitness and basal metabolic rate in community-dwelling middleaged women: a quasi-experimental study. Int J Environ Res Public Health, 2022, 19(23): 16157. [Crossref]
16. Carrasco-Poyatos M, Ramos-Campo DJ, & Rubio-Arias JA. Pilates versus resistance training on trunk strength and balance adaptations in older women: a randomized controlled trial. PeerJ, 2019, 7: e7948. [Crossref]
17. Liguori G ACoSM. ACSM's guidelines for exercise testing and prescription. Lippincott Williams & Wilkins, 2020.
18. Mänttäri A, Suni J, Sievänen H, Husu P, Vähä-Ypyä H, Valkeinen H, et al. Six-minute walk test: a tool for predicting maximal aerobic power (VO(2) max) in healthy adults. Clin Physiol Funct Imaging, 2018, 12525. [Crossref]
19. TAŞKIRAN Ö Ö Cİ, Golmoghani-Zadeh, N., A. AD, B. E, G. M, & A. F. Do Pilates and Yoga affect quality of life and physical performance of elderly living in a nursing home a preliminary study. Turkish Journal of Geriatrics/Türk Geriatri Dergisi, 2014, 17(3): 262-271.
20. Kloubec JA. Pilates for improvement of muscle endurance, flexibility, balance, and posture. J Strength Cond Res, 2010, 24(3): 661-667. [Crossref]
21. Pucci GCMF, Neves E, & Saavedra F. Effect of pilates method on physical fitness related to health in the elderly: a systematic review. Revista Brasileira de Medicina do Esporte, 2019, 25: 76-87. [Crossref]
22. Ruiz-Montero P J C-RA. Body composition, physical fitness and exercise activities of elderly. Journal of physical education and sport, 2016, 16(3): 860-870. [Crossref]
23. Oliveira LC, Oliveira RG, & Pires-Oliveira DA. Comparison between static stretching and the Pilates method on the flexibility of older women. J Bodyw Mov Ther, 2016, 20(4): 800-806. [Crossref]
24. Jubrias SA, Esselman PC, Price LB, Cress ME, & Conley KE. Large energetic adaptations of elderly muscle to resistance and endurance training. J Appl Physiol (1985), 2001, 90(5): 1663-1670. [Crossref]
25. Fernández-Rodríguez R, Álvarez-Bueno C, Ferri-Morales A, Torres-Costoso AI, Cavero-Redondo I, & MartínezVizcaíno V. Pilates method improves cardiorespiratory fitness: a systematic review and meta-analysis. J Clin Med, 2019, 8(11): 1761. [Crossref]
26. Fernandes IG, Macedo M, Souza MA, Silveira-Nunes G, Barbosa M, Queiroz ACC, et al. Does 8-week resistance training with slow movement cadenced by Pilates breathing affect muscle strength and balance of older adults? An age-matched controlled trial. Int J Environ Res Public Health, 2022, 19(17): 849-859. [Crossref]